EMR vs. EHR: Key Differences in Healthcare Technology
In healthcare technology, the terms EMR and EHR are often used interchangeably. They are related, but they are not always used to describe the same type of system. For therapy practices, understanding the difference matters because patient records are not just clinical files. They also connect to documentation, scheduling, billing, compliance, reporting, and care coordination.
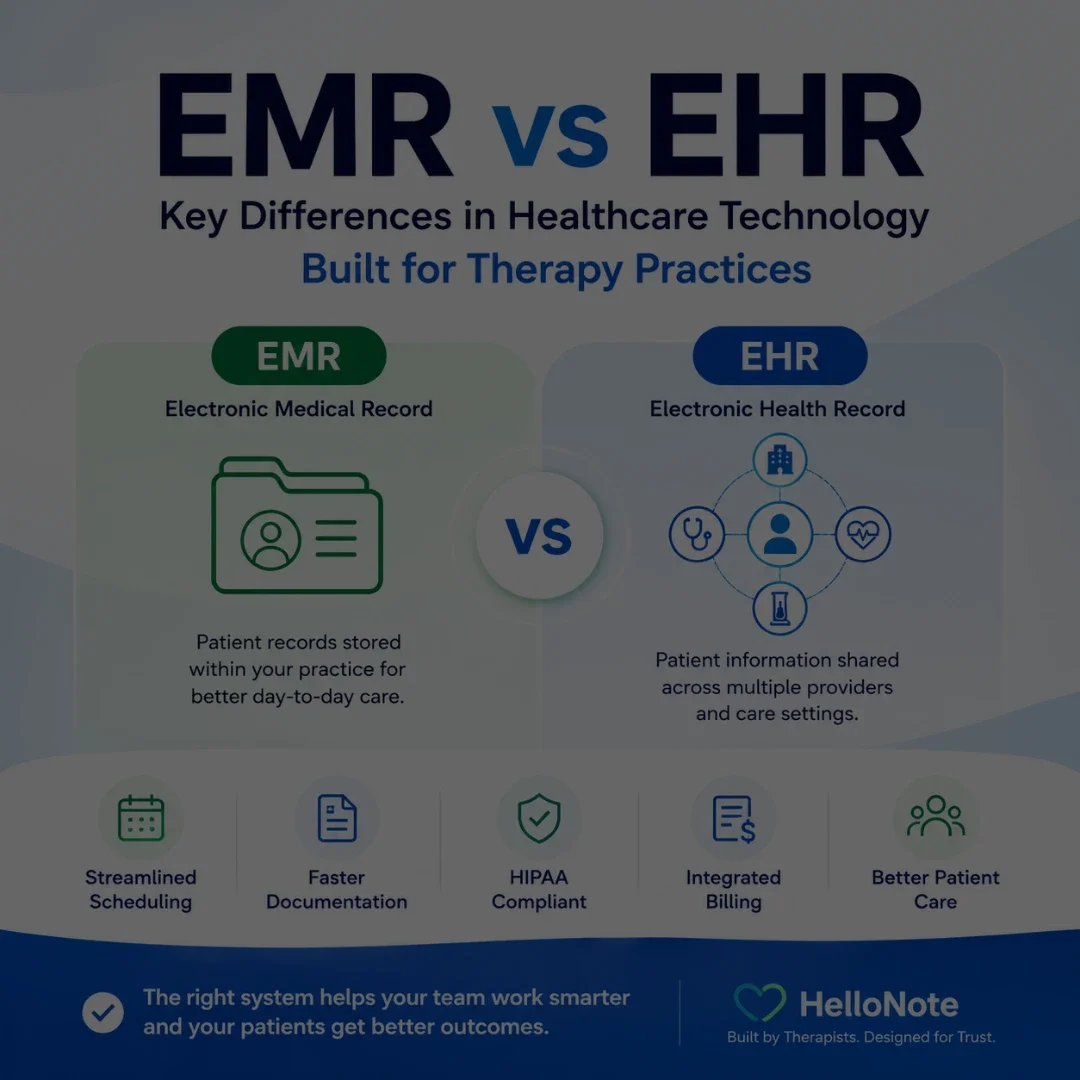
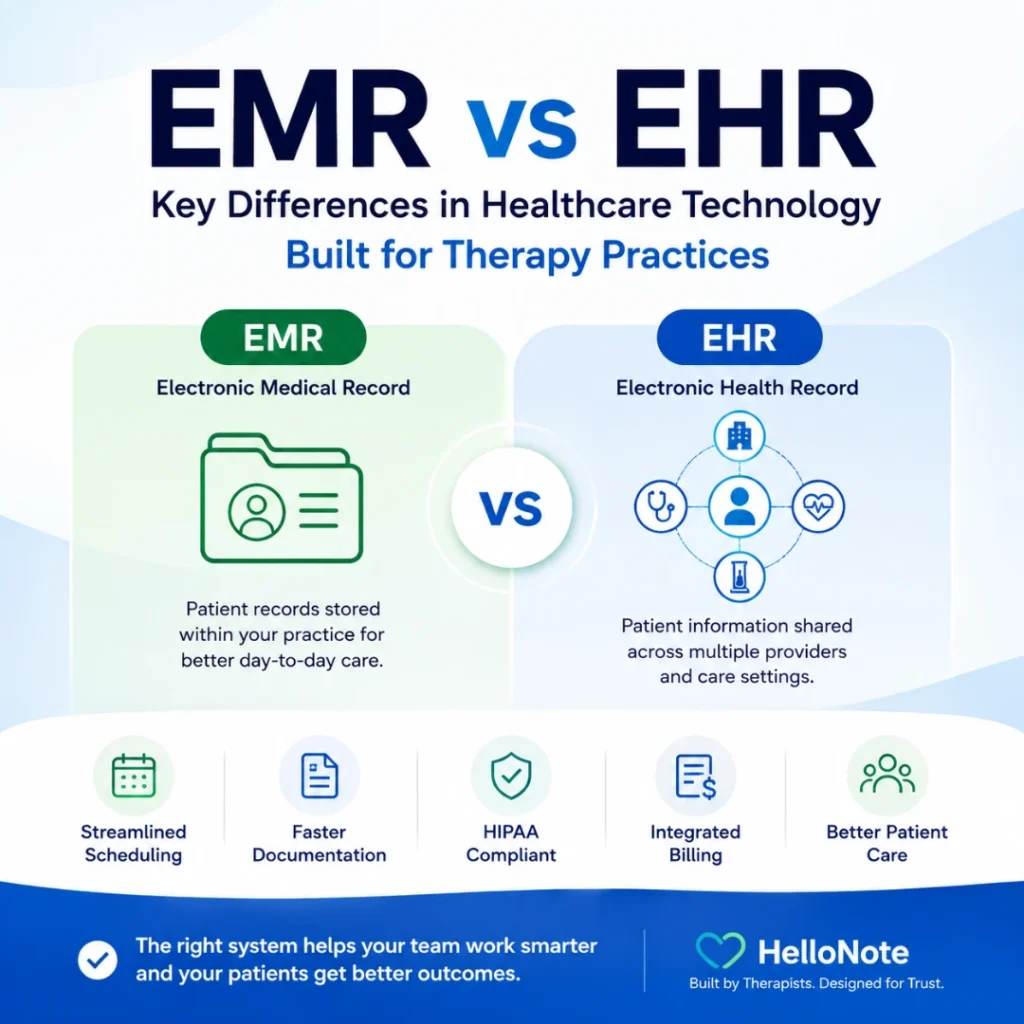
A physical therapy, occupational therapy, speech therapy, chiropractic, or behavioral health practice may use an EMR to manage day-to-day clinical and administrative workflows inside the practice. An EHR is typically broader and may support information sharing across multiple healthcare providers, such as physicians, hospitals, specialists, labs, and therapy clinics.
This article explains the practical difference between EMR and EHR systems, why the distinction matters for therapy practices, and what clinic owners should look for when choosing technology to support patient care and daily operations.
EMR vs EHR in one sentence
An EMR is generally a digital clinical record used within one practice, while an EHR is a broader health record designed to support care coordination and information sharing across multiple healthcare settings.
Table of Contents
Key Takeaways
- Pediatric therapy practices can grow revenue through services such as kids camps, caregiver workshops, screenings, assistive technology consulting, and telehealth.
- New income streams should support clinical goals, not distract from patient care.
- Community-based services can help practices build stronger relationships with families, schools, and referral partners.
- Practices need clear workflows for scheduling, documentation, payments, consent forms, reminders, and follow-up before adding new programs.
Understanding EMRs: What They Do
EMRs are often described as digital versions of your health history within a single healthcare practice, such as a therapy clinic. An EMR can include diagnoses, medications, treatment plans, progress notes, visit history, and other clinical details used by the provider managing the patient’s care.
For therapy practices, this means clinicians can quickly review patient history, update documentation, track progress over time, and make more informed treatment decisions during each visit.
What does an EMR do?
An EMR helps a healthcare practice store, manage, and update patient information inside one clinical system, including documentation, treatment history, appointment details, and other information needed for day-to-day care.
What Is an EHR?
An EHR, or Electronic Health Record, is a broader digital health record that may follow the patient across different healthcare settings. While an EMR is commonly centered on one practice, an EHR is typically designed to support information sharing between authorized providers and organizations involved in the patient’s care.
For example, an EHR may include information from a hospital, primary care provider, specialist, lab, imaging center, and therapy clinic. This broader view can help providers better understand the patient’s medical history and coordinate care across different parts of the healthcare system.
What does an EHR do?
The simplest way to understand EMR vs EHR is to look at scope. An EMR is often practice-centered. An EHR is usually patient-centered across a wider care network.
| Area | EMR | EHR |
|---|---|---|
|
Main purpose |
Digital record used within one practice or organization |
Broader health record shared across authorized providers and care settings |
|
Scope |
One clinic, practice, or organization |
Multiple healthcare settings, depending on interoperability and access |
|
Best use |
Daily documentation, treatment plans, scheduling, billing, and internal workflows |
Coordinated care and information exchange across providers |
|
Therapy example |
PT notes, OT goals, SLP progress, chiropractic documentation, visit history, and billing details |
Shared history from physicians, hospitals, specialists, labs, and therapy providers |
|
Data sharing |
Usually more practice-centered |
Designed for broader interoperability and continuity of care |
This distinction matters because therapy practices need both strong internal workflows and the ability to understand the patient’s broader care picture when coordination is needed.
Why EMR vs EHR Matters for Therapy Practices
A therapy-focused EMR can help a practice manage the clinical and administrative work that happens around every visit. The value is not only in storing records. The value is in connecting the record to the workflow.
- Streamlined documentation: Progress notes, treatment plans, patient details, and visit history are easier to manage in one system.
- Better progress tracking: Therapists can review prior visits, goals, outcomes, and plan-of-care updates over time.
- More efficient scheduling: Appointments, visit history, patient communication, and provider availability can stay connected.
- Billing support: Documentation and billing details can stay aligned so clinical and administrative teams are not working from separate records.
- Fewer manual handoffs: Clinicians, front desk staff, and billing teams can work from the same patient record instead of recreating information across multiple tools.
- Improved patient experience: Patient portals, intake forms, reminders, and communication tools can help reduce friction before and after each visit.
Looking for an EMR built for therapy practices?
HelloNote helps PT, OT, SLP, chiropractic, and behavioral health practices manage documentation, scheduling, billing, patient communication, and reporting in one connected system.
No credit card required · HIPAA Compliant · PT, OT & SLP
Where EHRs Help with Coordinated Care
EHRs become especially useful when a patient receives care from multiple providers. Therapy is often part of a larger care plan, and the therapist may need context from physicians, surgeons, neurologists, hospitals, labs, imaging centers, or other specialists.
For example, a speech therapist may need to understand a patient’s neurological history. A physical therapist may need post-operative details from an orthopedic surgeon. An occupational therapist may need information from a hospital discharge summary. In those cases, broader health information can support safer and more coordinated therapy decisions.
The goal is not to choose terminology for its own sake. The goal is to choose technology that gives the practice the information it needs to document accurately, communicate clearly, and support continuity of care.
Security, HIPAA, and Interoperability Considerations
Patient confidentiality is critical in any healthcare technology system. EMR and EHR systems should be designed with HIPAA compliance, secure access, role-based permissions, audit trails, and protected data handling in mind.
Interoperability also matters. In simple terms, interoperability means different healthcare systems can exchange and use information appropriately. Standards such as HL7 and FHIR are often part of this conversation because they help different systems communicate more consistently. A therapy practice does not need to become a technical standards expert, but it should understand whether the software it chooses can support secure data exchange when needed.
What should therapy practices know about EMR and EHR security?
Therapy practices should choose systems that support secure access, HIPAA-conscious workflows, role-based permissions, audit trails, and appropriate handling of protected health information.
Common EMR and EHR Challenges for Therapy Practices
EMR and EHR systems can improve workflows, but they can also create frustration when they are not designed around the way a therapy practice actually operates.
- Learning curve: Clinicians and staff may need training before they can use the system confidently.
- Cost considerations: Practices should understand what is included, what costs extra, and how pricing changes as the clinic grows.
- Data migration: Moving records from one system to another can require planning, review, and cleanup.
- Interoperability limits: Not every system connects easily with every other healthcare technology platform.
- Template fit: Generic systems may not support therapy-specific documentation as well as a therapy-focused EMR.
- Staff adoption: Even good software can fail when the team does not understand how it fits the workflow.
What Therapy Practices Should Look for in an EMR
When a therapy practice evaluates an EMR, the decision should go beyond whether the software can store records. The system should support the clinical, operational, billing, and patient-facing workflows that keep the practice moving.
- Therapy-specific documentation templates and customization options
- Scheduling tools that connect appointments to patient records
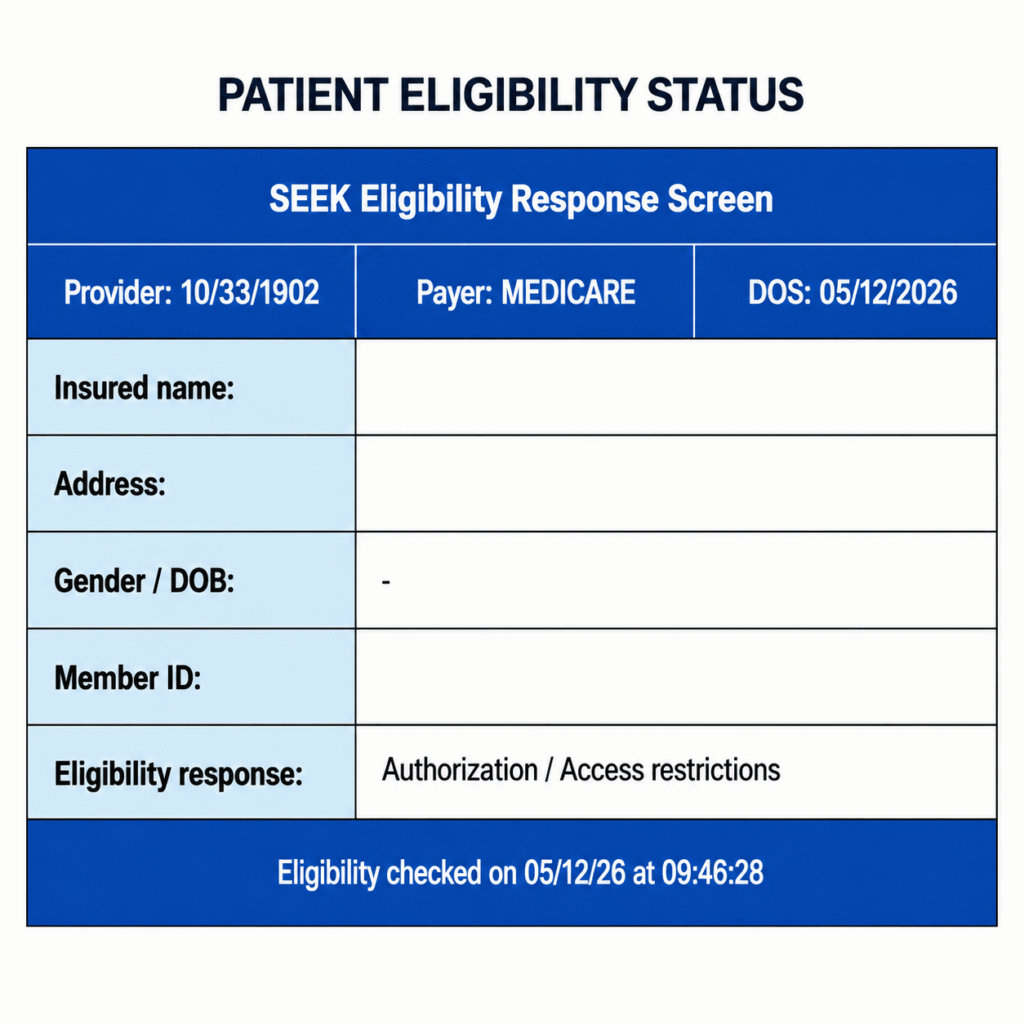
- Billing and eligibility workflows that align with documentation
- Patient portal, intake forms, and patient communication tools
- Authorization tracking and visit management
- Reports and analytics for practice visibility
- Multi-provider and multi-location support if the practice is growing
- Training, onboarding, and responsive support
- Security features that help protect patient information
How HelloNote Helps Therapy Practices Manage EMR Workflows
HelloNote is built for therapy practices that need more than a basic digital chart. By connecting documentation, scheduling, billing, patient communication, and reporting in one system, HelloNote helps PT, OT, SLP, chiropractic, and behavioral health practices manage day-to-day workflows more efficiently.
Instead of forcing clinicians and administrative teams to work from disconnected tools, HelloNote keeps the practice workflow connected. A patient record can support documentation, appointments, intake details, reminders, billing context, and reporting so the team has a clearer picture of what is happening across the practice.
For therapy practices, that connection matters. A record is not useful only because it stores information. It is useful because it helps the practice act on that information during patient care, scheduling, billing, and follow-up.
Practical Examples: EMR and EHR Use in Therapy Practices
The difference between EMR and EHR becomes easier to understand when it is applied to real therapy workflows.
- Physical therapy: A PT practice may use an EMR to track plan of care details, progress notes, visit frequency, authorization limits, and discharge planning.
- Occupational therapy: An OT may use an EMR to document functional goals, treatment activities, patient progress, and plan updates across sessions.
- Speech therapy: An SLP may use an EMR to review prior session notes, update therapy goals, document progress, and manage patient communication.
- Chiropractic care: A chiropractic practice may use an EMR to manage appointments, documentation, treatment history, billing details, and patient follow-up.
- Coordinated care: When a patient also sees a physician, surgeon, neurologist, or other provider, EHR-related information can help the therapy provider understand the broader care picture.
Frequently Asked Questions
What is the main difference between EMR and EHR?
An EMR is usually a digital patient record used within one healthcare practice or organization. An EHR is broader and is designed to support information sharing across multiple healthcare providers and care settings.
Do therapy practices use EMR or EHR systems?
Many therapy practices use EMR systems to manage documentation, scheduling, billing, patient communication, and daily practice workflows. Some systems may also support broader EHR-related functions, depending on interoperability and information sharing needs.
Why does EMR vs EHR matter for therapists?
The difference matters because therapists need accurate patient records for documentation, progress tracking, plan-of-care updates, billing support, and coordinated care. Understanding the difference helps practices choose software that fits their actual workflow.
Can an EMR help with scheduling and billing?
Yes. A therapy-focused EMR can support scheduling, documentation, billing, eligibility, authorizations, reminders, and patient communication. The strongest systems connect these workflows instead of keeping them separate.
What should therapy practices look for in an EMR system?
Therapy practices should look for documentation tools, scheduling, billing support, patient portal features, intake forms, reporting, security features, training, support, and workflows designed for PT, OT, SLP, chiropractic, or behavioral health care.
Is HelloNote an EMR for therapy practices?
Yes. HelloNote is an EMR and practice management platform built for therapy practices, including PT, OT, SLP, chiropractic, and behavioral health workflows. It helps practices manage documentation, scheduling, billing, patient communication, and reporting in one connected system.
Final Thoughts
EMR and EHR systems both play important roles in healthcare technology, but the difference matters most when it affects how a practice actually works. For therapy practices, the record is not just a file. It is part of the workflow that supports documentation, scheduling, billing, patient communication, compliance, and care coordination.
An EMR can help a therapy practice organize and manage the information it uses every day. An EHR can support a broader view of the patient’s health information when multiple providers are involved. The right system should make both clinical care and practice operations easier to manage.
If your current system makes documentation harder, separates scheduling from billing, or forces your team to repeat the same information across multiple tools, it may be time to look at a more connected therapy EMR.
Have questions about choosing the right EMR for your therapy practice?
HelloNote is built by therapists to help PT, OT, SLP, and Chiro practices manage documentation, scheduling, billing, and patient workflows in one connected system.
No credit card required • HIPAA Compliant • PT, OT & SLP