Clearinghouse Strategy for Therapy Practices: What PT, OT, and SLP Need to Know in 2026

What does a clearinghouse do for therapy billing and why does it matter?
The best clearinghouse for medical billing is an intermediary service that receives claims from your therapy EMR, formats them to meet each insurance payer’s specific requirements, scrubs them for errors, and transmits them securely via Electronic Data Interchange (EDI) to the insurance company. For physical therapy, occupational therapy, and speech-language pathology practices, the clearinghouse directly affects how fast claims are processed, how often they are rejected, and how quickly Electronic Remittance Advice (ERA) returns to your billing system. The wrong clearinghouse for your payer mix creates claim rejections and revenue delays that compound over time.
Key Takeaways
- HelloNote gives therapy practices two ways to pay for the EMR: per-user pricing and per-note pricing.
- Per-user pricing can work well for clinics with predictable staffing and consistent patient volume.
- Per-note pricing may be useful for part-time therapists, solo providers, mobile clinicians, and practices with changing caseloads.
- HelloNote’s current pricing calculator displays a $99 base price and separate note rates based on the selected option.
- High-volume practices producing more than 4,000 notes per month can contact HelloNote to discuss enterprise pricing.
- The right EMR pricing model should match the way your clinic works today and leave room for growth.
For physical therapy, occupational therapy, and speech-language pathology practices, clearinghouse selection is one of the most consequential billing decisions you will make in 2026. A therapy billing clearinghouse is the infrastructure that carries your claims from HelloNote to insurance payers, and the performance of that infrastructure directly determines how fast you get paid, how often claims come back rejected, and how much administrative time your billing team spends chasing down errors.
HelloNote was built with a specific philosophy on this: your practice should never be locked into a single clearinghouse with poor performance. That is why HelloNote integrates with multiple clearinghouse partners and gives you the flexibility to choose and switch based on your payer mix. In 2026, with payer requirements continuing to shift and claim scrutiny higher than it has ever been, having a clearinghouse strategy is not optional. It is a core part of running a financially healthy therapy practice.
This guide covers what clearinghouses do, which partners HelloNote works with, how automated claim submission changes the revenue cycle in 2026, and how to choose the right clearinghouse for your specific payer mix.
What Is a Clearinghouse and Why Does It Matter for Therapy Billing
What is a clearinghouse in medical billing? A clearinghouse sits between your billing software and the insurance companies that pay your claims. Its job is to take the claims you generate in HelloNote, translate them into the format each payer requires, check them for errors before they reach the insurance company, and deliver them securely. When the insurance company responds with payment or denial information, the clearinghouse brings those remittances back into HelloNote.
For therapy practices, even small errors on a claim can trigger a denial that delays payment by weeks. A missing therapy discipline modifier, an incorrect place of service code, or an expired prior authorization number are the kinds of errors that a good clearinghouse catches before the claim ever reaches the payer. The clearinghouse is your last line of defense against preventable denials.
Data Formatting
Insurance companies have different formatting requirements for claim submission. Medicare uses different specifications than Blue Cross, and commercial payers vary from each other. A clearinghouse converts every claim from HelloNote into the specific format each payer requires, eliminating the need for your billing team to manage those differences manually.
Claim Scrubbing
Before sending a claim to the payer, the clearinghouse runs it through a scrubbing process that checks for common errors: missing modifiers, incorrect codes, incomplete patient information, expired authorizations, and payer-specific rule violations. Claims that fail scrubbing are returned to HelloNote with an error description so the billing team can correct and resubmit. Catching errors at this stage costs far less time than resolving a payer denial after the fact.
Secure EDI Claims Data Exchange
Clearinghouses transmit claims using Electronic Data Interchange (EDI), the standardized format that HIPAA requires for electronic claim submission. EDI transmission is encrypted and auditable, creating a secure and documented pathway for protected health information between your practice and payers. Without a clearinghouse, practices would need to establish direct EDI connections with each individual payer, which is operationally not feasible for most therapy practices.
Electronic Remittance Advice
When a payer processes a claim, it sends an Electronic Remittance Advice (ERA) back through the clearinghouse. The ERA contains payment information, denial reason codes, and adjustment details. HelloNote’s clearinghouse integration automatically syncs ERA files into the billing system, eliminating manual payment posting and accelerating the reconciliation process.

HelloNote Clearinghouse Integrations in 2026
HelloNote integrates with multiple clearinghouse partners, giving therapy practices the flexibility to choose based on payer mix, claim volume, and specific operational needs. The following clearinghouses are currently integrated with HelloNote.
Inovalon
Inovalon is one of HelloNote’s primary clearinghouse partners and is the preferred Inovalon clearinghouse option for practices with a Medicare-heavy payer mix. Inovalon provides extensive payer connectivity, including robust Medicare eligibility verification and claim submission capabilities. The integration is well-established within HelloNote, and the enrollment process is straightforward.
For practices migrating from a previous EMR that used Inovalon, the transition to HelloNote does not require starting the enrollment process from scratch. Contact your Inovalon account manager and request a transfer to destination ID 589187 (E Medical Records Live Inc.). This preserves your existing payer enrollments and minimizes setup time.
Trizetto
Trizetto is a strong Trizetto clearinghouse option for practices with a diverse commercial payer mix. Trizetto offers broad connectivity with commercial insurance companies and can deliver better acceptance rates for specific commercial payers than other clearinghouse options. If your practice bills to multiple commercial insurers and experiences frequent rejections through your current clearinghouse, Trizetto is worth evaluating as an alternative.
ClaimMD
ClaimMD is an additional clearinghouse option integrated with HelloNote, particularly useful for practices that need cost-effective commercial payer connectivity. Like Trizetto, ClaimMD can be evaluated against your specific payer mix to determine whether it outperforms your current clearinghouse for the insurers you bill most frequently.
Clearinghouse Switching Flexibility
Unlike EMRs that lock practices into a single clearinghouse regardless of performance, HelloNote allows you to select and switch clearinghouses based on results. If your current clearinghouse experiences downtime, processing delays, or consistently poor performance with a specific payer, you can migrate to a different partner without changing your EMR. This flexibility gives you leverage to demand better service and ensures your revenue cycle is never held hostage by a single vendor.
Your clearinghouse strategy starts with the right EMR.
HelloNote integrates with Inovalon, Trizetto, and ClaimMD. Choose the best option for your payer mix, or switch if performance drops. No setup fees. No contracts.
No credit card required · HIPAA Compliant · PT, OT & SLP
New in 2026: Automated Claim Submission Workflows
How does automated claim submission work in HelloNote in 2026?
In 2026, HelloNote can be configured to handle the entire claim submission process automatically. When a therapist finalizes a note, HelloNote scrubs the claim for errors. If no errors are found, the claim is sent directly to the clearinghouse. If the clearinghouse also finds no issues, HelloNote releases the claim to the payer without any manual intervention. Only claims with errors require review. This workflow eliminates the human delays between note finalization and claim submission, reducing days in accounts receivable by 3 to 7 days. The feature is not enabled by default and must be activated through HelloNote support.
One of the most significant billing updates in HelloNote for 2026 is the expansion of automated claim submission capabilities. Previously, many practices manually reviewed and released claims from the clearinghouse queue after scrubbing. The new workflow eliminates that manual step for clean claims.
How the Automated Workflow Operates
- Therapist finalizes a note in HelloNote
- HelloNote automatically scrubs the claim for errors
- If no errors are found, the claim is sent directly to the clearinghouse
- If the clearinghouse also finds no issues, HelloNote auto-releases the claim to the payer
- Only claims with errors require manual review in Billing > Claims > Ready to Send
Revenue Cycle Impact
This workflow reduces days in accounts receivable by eliminating human delays between note finalization and claim submission. For a busy therapy practice seeing 20 or more patients per day, the difference between submitting claims on the same day as the visit versus 1 to 3 days later has a direct and measurable impact on cash flow. The 3 to 7 day reduction in accounts receivable translates to faster access to revenue that would otherwise sit in the billing pipeline.
How to Enable Automated Claim Submission
The automated claim submission feature is not enabled by default in HelloNote. Contact HelloNote support to activate it for your account. Once enabled, the system transforms your billing workflow from reactive manual review to automated submission with exception handling, where your billing team focuses exclusively on the claims that need attention rather than processing every claim individually.
How to Choose the Right Clearinghouse for Your Practice
Not all clearinghouses perform equally for every payer. The best clearinghouse for medical billing in a therapy practice depends on your specific payer mix, your claim volume, and whether you have existing payer enrollments to preserve. Here is how to evaluate the options.
Medicare-Heavy Practices
Inovalon has strong Medicare connectivity and is typically the best-performing option for practices that bill primarily to Medicare Part B. The enrollment process through HelloNote is well-established, and the integration supports Medicare eligibility verification, claim submission, and ERA processing within a single workflow.
Commercial Payer-Heavy Practices
Trizetto or ClaimMD may offer better acceptance rates for specific commercial insurers. If your practice bills to multiple commercial payers and your current clearinghouse is generating frequent rejections for a specific insurer, testing a different clearinghouse for that payer is worth the effort. HelloNote’s multi-clearinghouse flexibility allows you to run different clearinghouses for different payer groups if the data supports it.
Practices With Existing Clearinghouse Accounts
If you have an existing clearinghouse account from a previous EMR, HelloNote allows you to transfer that account rather than starting the enrollment process from scratch. This is particularly valuable for practices that have spent months building out payer enrollments. Preserving those enrollments during an EMR migration eliminates weeks of setup time and ensures no interruption to claim submission during the transition.
| Clearinghouse | Best For | Key Strength | HelloNote Integration |
|---|---|---|---|
|
Inovalon |
Medicare-heavy practices |
Strong Medicare connectivity and eligibility verification |
Primary partner, well-established |
|
Trizetto |
Commercial payer mix |
Broad commercial payer connectivity |
Available, evaluate against your payer mix |
|
ClaimMD |
Cost-effective commercial billing |
Strong commercial payer acceptance rates |
Available, evaluate against your payer mix |
Enrollment Timelines and Operational Planning

Setting up a new clearinghouse through HelloNote typically takes 5 to 10 business days. This includes payer enrollment, testing, and validation. During this period, claims can still be submitted manually or through existing arrangements, so there is no gap in claim submission during the setup window.
Planning a Clearinghouse Transition
For practices switching clearinghouses, the transition can be planned during a lower-volume period to minimize disruption. HelloNote’s support team can help coordinate the transfer and verify that no claims are lost or duplicated during the transition. Before switching, document your current payer enrollment list so the new clearinghouse setup covers every active payer without gaps.
Eligibility Verification During Setup
Real-time eligibility verification depends on clearinghouse connectivity. Before you verify a patient’s Medicare or commercial insurance benefits, the clearinghouse must have an active connection to that payer. During clearinghouse setup, eligibility verification for specific payers may be limited until enrollment completes. Plan patient scheduling around this window to avoid verification delays at the front desk.
Auto-ERA Activation
Once clearinghouse enrollment is complete, enable Auto-ERA functionality in HelloNote. ERA files will automatically sync from the clearinghouse into HelloNote under Billing > Import > ERA/835. This automation eliminates manual payment posting and accelerates the reconciliation process. If ERA files are not appearing after enrollment, contact HelloNote support to verify the ERA auto-sync configuration.
Common Clearinghouse Issues and How to Resolve Them
Even with a well-configured clearinghouse, therapy practices encounter billing issues. Here are the most common problems and their resolutions.
Claim Rejection Due to Missing Modifiers
The most common cause of claim rejection in therapy billing is a missing discipline modifier. PT claims require modifier GP, OT claims require modifier GO, and SLP claims require modifier GN. HelloNote’s claim scrubbing catches many of these, but payer-specific rules may require additional modifier review. If a specific payer is generating repeated modifier rejections, review that payer’s modifier requirements and update the claim template in HelloNote accordingly.
ERA Not Syncing Into HelloNote
If Electronic Remittance Advice files are not appearing in HelloNote under Billing > Import > ERA/835, the clearinghouse ERA connection may need to be revalidated. This can happen after a clearinghouse system update or if the enrollment configuration changes. Contact HelloNote support to check the ERA auto-sync configuration and reestablish the connection if needed.
Delayed Claim Acceptance
If claims are taking longer than expected to show as accepted by the clearinghouse, check the Submitted tab under Billing > Claims. This view shows claims sorted by billed amount, paid status, hold status, and submission date, giving your billing team full visibility into where delays are occurring. Claims held in a pending status at the clearinghouse often indicate a payer-specific connectivity issue that may require a temporary manual submission while the connection is restored
Payer-Specific Connectivity Gaps
Not every clearinghouse connects to every payer with equal performance. If your practice experiences frequent rejections from a specific insurance company, the issue may be that your current clearinghouse has limited connectivity with that payer. Review the rejection pattern: if rejections are concentrated on one or two payers, consider switching to a clearinghouse with stronger connectivity for those specific payers. HelloNote’s multi-clearinghouse flexibility makes this a practical option without requiring a full clearinghouse migration.
Formatting Errors After Payer Rule Changes
Insurance payers periodically update their claim formatting requirements, often without advance notice to providers. If claims that were previously accepted begin rejecting for formatting errors, the clearinghouse may not have updated its payer rules yet. Contact your clearinghouse support team to confirm whether a payer rule update is pending. In the interim, manual review of affected claims before submission can prevent denials while the clearinghouse update is applied.
Is It Better to Switch Clearinghouses or Fix the Current One?
It depends on whether the problem is isolated or systemic. If rejections are concentrated on one or two specific payers, the issue is usually a connectivity gap with your current clearinghouse for those payers specifically, not a reason to replace the whole relationship. If rejections are broad, frequent, and span multiple payers, that points to a deeper performance problem worth switching over. HelloNote’s multi-clearinghouse flexibility means you do not have to choose one or the other. You can run a different clearinghouse for a specific payer group without a full migration.
How HelloNote Simplifies Clearinghouse Management
HelloNote’s approach to clearinghouse medical billing integration is built on a single principle: your billing software should work for your practice, not create additional administrative burden. Here is how that principle is implemented in the platform.
One-Click Claim Submission
Once a claim is finalized and scrubbed in HelloNote, sending it to the clearinghouse requires a single click. There is no file exporting, no manual formatting, and no uploading to a separate portal. The entire submission workflow lives inside HelloNote, keeping your billing team in one system from note finalization through payment posting.
Centralized Claim Tracking
The Submitted tab under Billing > Claims provides a complete view of every claim in the pipeline. Sort by date, status, billed amount, or payer to identify bottlenecks and prioritize follow-up. This centralized view eliminates the need to log into the clearinghouse portal separately to check claim status, saving your billing team time on every working day.
Automatic ERA Processing
When remittances arrive from the clearinghouse, HelloNote can automatically post payments to the correct patient accounts. This eliminates manual data entry for payment posting and reduces the risk of posting errors that create reconciliation problems later. Practices that enable automatic ERA processing typically see a significant reduction in the time their billing team spends on payment reconciliation.
Flexible Clearinghouse Switching
If a clearinghouse underperforms, you can switch. HelloNote does not lock your practice into a single vendor. This flexibility gives you leverage to demand better service from your clearinghouse partner and ensures your revenue cycle is not dependent on the performance of a single vendor relationship. For therapy practices with multiple locations or diverse payer mixes, the ability to run different clearinghouses for different payer groups provides a level of billing optimization that single-clearinghouse EMRs cannot match.
Still chasing claim rejections your clearinghouse should have caught?
HelloNote connects to Inovalon, Trizetto, and ClaimMD, so your practice can pick the best clearinghouse for medical billing based on your actual payer mix. Start free and see how it works for PT, OT, SLP, and Chiro.
No credit card required • HIPAA Compliant • PT, OT & SLP
Frequently Asked Questions
What is a clearinghouse in therapy billing?
A medical billing clearinghouse is an intermediary service that sits between your therapy EMR and insurance payers. It receives claims from HelloNote, formats them to meet each payer's specific requirements, scrubs them for errors, and transmits them securely via EDI. When payers respond with payment or denial information, the clearinghouse delivers Electronic Remittance Advice (ERA) back to HelloNote. The clearinghouse directly affects how fast your claims are processed and how often they are rejected.
Which clearinghouse does HelloNote use?
HelloNote integrates with multiple clearinghouses including Inovalon, Trizetto, and ClaimMD. The best choice depends on your payer mix. Inovalon is typically best for Medicare-heavy practices. Trizetto and ClaimMD offer strong commercial payer connectivity and may perform better for practices with diverse commercial insurance mixes. HelloNote allows you to switch clearinghouses if performance does not meet your needs.
How long does clearinghouse setup take with HelloNote?
Setting up a new clearinghouse through HelloNote typically takes 5 to 10 business days, including payer enrollment, testing, and validation. Practices migrating from a previous EMR that already used Inovalon can transfer their existing account to HelloNote by contacting their Inovalon account manager and requesting a transfer to destination ID 589187. This preserves existing payer enrollments and reduces setup time.
What is automated claim submission and how does it reduce accounts receivable?
Automated claim submission in HelloNote 2026 allows the system to send clean claims directly from note finalization to the clearinghouse and on to the payer without any manual intervention. Only claims with errors require review. This eliminates the human delays between note finalization and claim submission, reducing days in accounts receivable by 3 to 7 days. The feature must be enabled by contacting HelloNote support.
Why are my therapy claims being rejected by the clearinghouse?
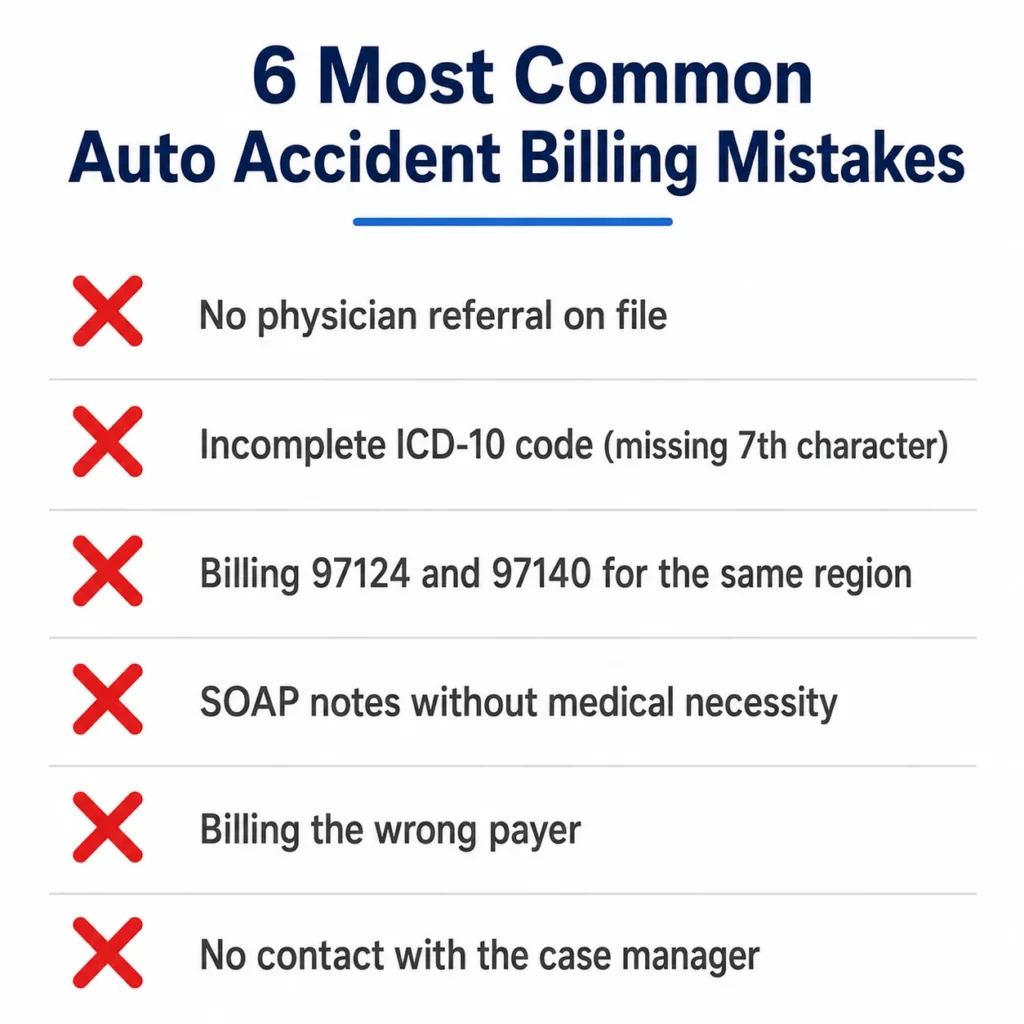
The most common causes of therapy claim rejections at the clearinghouse are missing discipline modifiers (GP for PT, GO for OT, GN for SLP), incorrect place of service codes, missing prior authorization numbers, and incomplete patient information. HelloNote's claim scrubbing catches many of these errors before submission, but payer-specific rules may require additional review. If rejections are concentrated on one payer, the issue may be a connectivity gap between your clearinghouse and that specific insurer.
Can I switch clearinghouses without changing my EMR?
Yes. HelloNote does not lock your practice into a single clearinghouse. If your current clearinghouse underperforms, experiences downtime, or has poor connectivity with a specific payer, you can switch to a different clearinghouse partner within HelloNote without changing your EMR or disrupting your overall billing workflow. This flexibility is a core feature of HelloNote's billing architecture.