
What is CPT 97530 (Therapeutic Activity)?
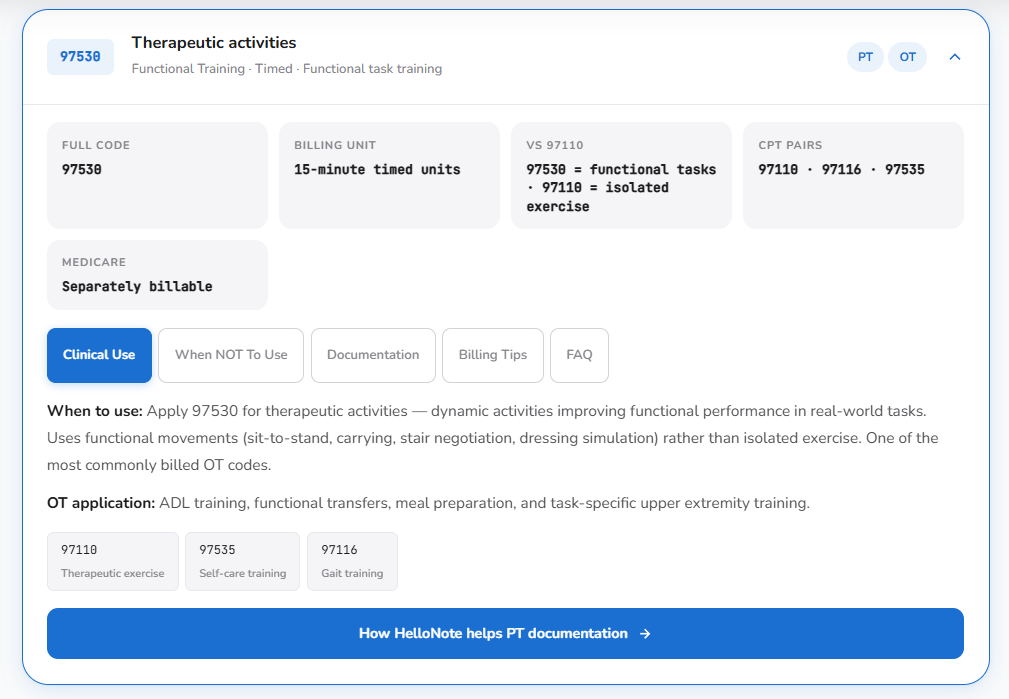
CPT 97530 is a timed therapeutic procedure code for therapeutic activities — dynamic, functional tasks that simulate real-life activities of daily life. Billed in 15-minute units, it requires direct one-on-one licensed therapist contact throughout. It applies when the clinical goal is improving functional performance, not an isolated impairment like strength or range of motion.
Key Takeaways
- CPT 97530 covers functional, multi-outcome activities that simulate real-life tasks — billed in 15-minute units with direct therapist contact required throughout
- The clinical anchor is functional performance: the activity must resemble what the patient needs to do in their daily life, not target an isolated musculoskeletal impairment
- 97530 and 97110 serve different clinical purposes and can be billed together — but each requires its own time tracking and its own documented clinical justification
- HelloNote’s 97530 template enforces the functional goal connection and multi-outcome documentation that payers look for — making the defensible note the default note
Table of Contents
CPT 97530 is the most searched therapy billing code on the HelloNote site. It is also the code our billing team sees questioned most often in payer reviews. Those two facts are not a coincidence — they reflect a gap that runs through outpatient therapy documentation everywhere. Therapists use 97530 constantly because the clinical reality of functional rehabilitation is constantly functional. Payers scrutinize it constantly because the documentation that supports it is rarely as specific as the clinical work it is supposed to describe.
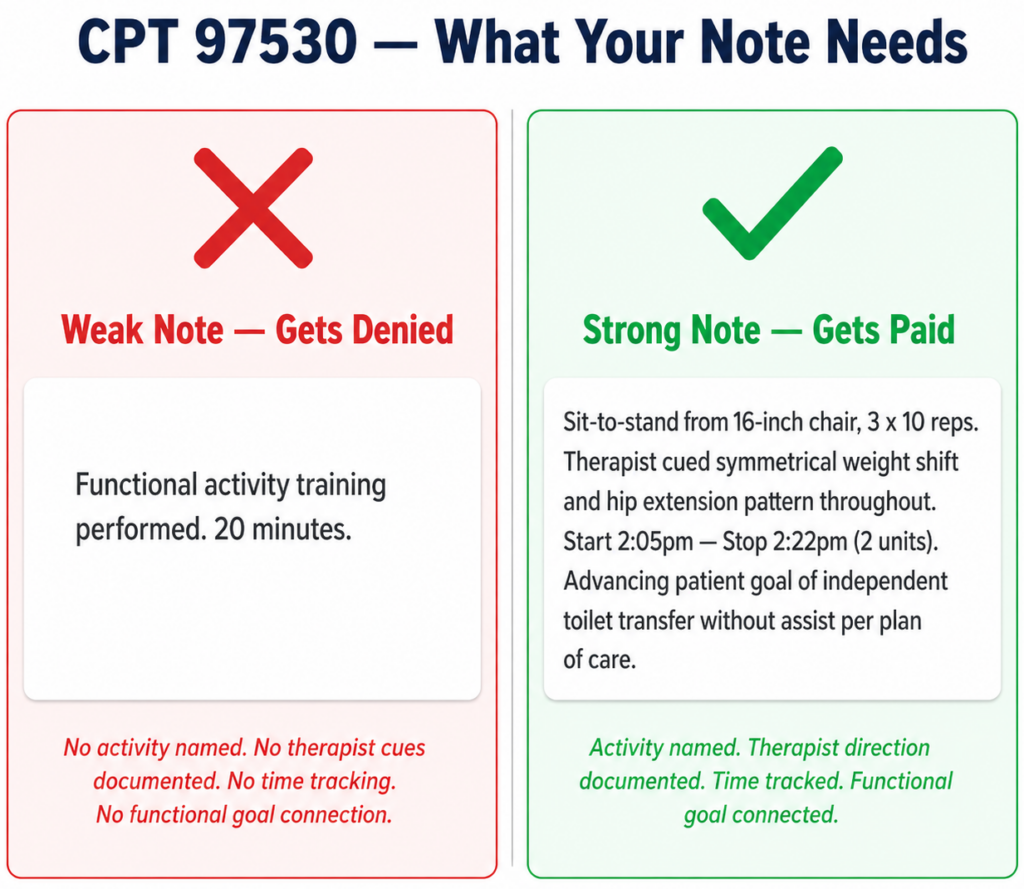
The code is not the problem. The definition is straightforward: dynamic activities to improve functional performance, direct one-on-one contact, 15-minute units. The problem is the space between what happens in the room and what ends up in the note. A therapist guides a patient through a kitchen simulation task that integrates balance, upper extremity coordination, cognitive sequencing, and ADL independence in one twenty-minute session. The note says “functional activity training, 20 minutes.” The clinical work was skilled and complex. The documentation is barely defensible.
This guide is the version of the 97530 conversation that actually helps: what the code requires clinically, what documentation payers need to approve it, how it differs from 97110, and exactly how our team structures every 97530 note so it reflects what we did and withstands what auditors look for. We also address the 97110 vs 97530 comparison at a structural level here — for the full side-by-side breakdown, our complete guide lives at hellonote.com/97110-vs-97530/.

What Is CPT 97530 — The Clinical Definition That Actually Matters
The AMA defines CPT 97530 as: therapeutic activities, direct (one-on-one) patient contact by the provider, use of dynamic activities to improve functional performance, each 15 minutes. Three words in that definition carry the most clinical weight: dynamic, functional, and direct.
Dynamic
The patient is actively performing movement — not being moved by the therapist. The activity requires patient effort, coordination, and engagement across multiple systems simultaneously. This distinguishes 97530 from manual therapy codes where the therapist does the work.
Functional
The activity mirrors something the patient needs to do in their real life. Not an isolated exercise targeting a single tissue or movement direction — a task with the multi-joint, multi-outcome complexity of daily living. This is the clinical anchor that separates 97530 from 97110.
Direct
The licensed therapist must be present and actively directing the activity for the entire billed duration. Not supervising from across the room. Not setting up and stepping away. Direct contact, direct instruction, direct skilled input throughout. If the activity could be run by a tech or continued as a home program without skilled therapist presence — the documentation needs to explain why it was not.
What CPT 97530 Covers
Therapeutic activities under 97530 include functional mobility training such as sit-to-stand practice, transfer training, stair negotiation, and community ambulation on varied surfaces. ADL task practice including meal preparation simulation, upper extremity reaching and manipulation tasks in functional contexts, dressing and grooming sequences, and home management activities. Work simulation tasks for return-to-work clearance. Sport-specific movement pattern practice for athletic return. Pediatric functional play and developmental activity sequences requiring skilled therapist direction and progressive challenge.
What CPT 97530 Does Not Cover
97530 is not appropriate for isolated therapeutic exercise targeting a single tissue capacity (use 97110). It is not appropriate for gait training as a standalone skilled service (use 97116). It is not appropriate for patient education where the therapist explains or demonstrates rather than directly guides active patient performance. It is not appropriate when the activity is performed without continuous direct therapist contact. The activity has to be functional, the patient has to be doing it, and the therapist has to be directing it throughout.
When to Use CPT 97530: The Functional Performance Standard
The functional performance standard is the clinical test our team applies before every 97530 billing decision. It has two parts. First: does this activity resemble something the patient needs to perform in their daily life? Second: does the therapeutic value of this activity come from its functional, multi-outcome complexity rather than its impact on a single measurable tissue capacity?
If both answers are yes — the code is 97530. If the second answer is no — if the therapeutic value is primarily a strength gain, a ROM increase, or an endurance improvement that happens to occur during a functional-looking activity — the code is 97110, and the documentation needs to reflect that single-outcome intent.
The Multi-Outcome Principle
97530 activities work across multiple systems simultaneously. A sit-to-stand sequence builds lower extremity loading tolerance, reinforces hip and knee proprioception, challenges dynamic balance, practices the movement pattern used in every functional transfer, and advances the documented goal of independent toilet and chair use. Six things changing at once. That is not a 97110 intervention. The multi-outcome nature of the activity is what makes it 97530 — and that multi-outcome nature needs to appear in the documentation.
Populations and Diagnoses That Fit 97530
Post-surgical orthopedic patients transitioning from impairment-level work to functional task practice: hip and knee arthroplasty patients practicing transfers and stair negotiation, shoulder repair patients practicing reaching and lifting in functional contexts, hand patients practicing grip and manipulation tasks in ADL simulations. Neurological patients practicing multi-step ADL sequences: stroke survivors relearning dressing and grooming, TBI patients practicing kitchen tasks, Parkinson’s patients working on functional gait in environmental simulations. Older adults with fall risk practicing functional mobility in community simulation environments. Work injury patients performing job-specific task simulations for return-to-work clearance.
CPT 97530 Documentation Requirements
97530 documentation fails in a predictable pattern. The therapist records the activity accurately and omits the functional goal it was designed to advance. Functional reaching practice, 15 minutes. Step training, 3 sets. Kitchen simulation, direct therapist contact. These notes describe what happened. They do not establish medical necessity, and they do not tell a payer why a licensed therapist needed to direct the activity rather than delegating it to support staff or a home program.
Our team rebuilt our 97530 documentation standard around four required elements. Every 97530 note we write contains all four.
The Four Required Documentation Elements
- The specific activity and its multi-outcome components
Name the activity specifically and describe its functional complexity. Not ‘stair training performed’ but ‘reciprocal stair negotiation with handrail, 3 x 8 steps ascending and descending, targeting lower extremity loading tolerance, dynamic balance, and hip extension mechanics required for safe community stair use.’ The multi-outcome description is what makes the note reflect a 97530 activity rather than a 97110 exercise.
- The skilled therapist direction throughout
Document the specific cues, modifications, and clinical decisions made during the activity. What did the therapist observe that required skilled input? What cue improved performance? What modification was made in response to the patient’s real-time performance? This element establishes that direct skilled contact occurred and that the intervention required professional direction.
- Actual start and stop time
The 8-minute rule applies to 97530 exactly as it does to 97110. One unit requires at least 8 minutes of direct therapist contact. Document actual times, not estimates. When billing 97530 and 97110 on the same visit, each code needs its own time block documented separately.
- The functional goal connection sentence
Connect every 97530 activity to a documented functional goal in the plan of care. This sentence establishes medical necessity. Example: ‘Kitchen simulation task practice targeting the patient’s goal of independent hot meal preparation within her home environment following right hip arthroplasty.’ Without this connection the documentation describes an activity program. With it, it establishes a medically necessary skilled rehabilitation service.
CPT 97530 vs CPT 97110: The One Distinction That Protects Your Claims
CPT 97530 vs 97110: What is the difference?
CPT 97110 targets a single musculoskeletal impairment — strength, endurance, ROM, or flexibility — through isolated therapeutic exercise. CPT 97530 targets functional performance through multi-outcome activities that simulate real-life tasks. 97110 changes a tissue capacity. 97530 changes what the patient can do. The distinction is clinical intent, which must be documented explicitly in the note.
The System Being Treated
97110 treats a musculoskeletal impairment. The target is a specific deficit in tissue capacity. The outcome is measured in tissue-level numbers: MMT grade, goniometric degrees, repetitions to fatigue. 97530 treats a functional performance deficit. The target is the patient’s ability to perform a specific task. The outcome is measured in functional terms: the patient can now ascend stairs safely, prepare a meal independently, return to their work duties.
The Sticky Note Test
Our team uses a simple test when code selection is unclear. Ask: if this intervention worked perfectly, what one thing would be different? If the answer is a tissue capacity measurement — the quad is stronger, the shoulder moves further — that is 97110. If the answer is a functional task — the patient can get off the floor independently, return to their job, prepare a meal — that is 97530. Document the answer. That is your code justification.
Billing CPT 97530 on the Same Day as 97110: Rules and Modifier 59
Billing 97110 and 97530 on the same day is appropriate, clinically sound, and common in well-structured outpatient sessions. The sequence is logical: therapeutic exercise builds the impairment-level capacity (97110), and therapeutic activity practices the functional task that capacity enables (97530). Strengthen the quad, then practice the stair negotiation that quad strength supports.
What Makes Same-Day Billing Defensible
Each code needs its own documented time block with separate start and stop times. Each code needs its own clinical justification establishing a distinct therapeutic purpose. The combined documentation should tell a coherent clinical story where the 97110 impairment and the 97530 functional task are clearly connected. When these conditions are met, same-day billing is not an audit flag. It is accurate documentation of a complete rehabilitation session.
Modifier 59 for CPT 97530
Some payers require Modifier 59 when 97110 and 97530 are billed on the same day to confirm they represent distinct and separately identifiable services. When required, the documentation must provide the clinical distinction the modifier signals — the modifier tells the payer these are separate services; the notes prove it. Verify Modifier 59 requirements with each payer as requirements vary by insurer.
Looking up more cpt codes?
See 97110, 97530, and 50+ therapy procedure codes – with billing guidance and documentation tips in one place.
Common Billing Mistakes with CPT 97530
Mistake 1 — Using 97530 for Impairment-Level Exercise
The most common misapplication: applying 97530 to exercises that are 97110 interventions because they happen in a functional position or involve multiple joints. A standing exercise is not automatically a functional activity. The test is always clinical intent: is the therapist targeting tissue capacity (97110) or functional task performance (97530)? If tissue capacity, bill 97110 regardless of how the exercise looks.
Mistake 2 — Missing the Functional Goal Connection
97530 without an explicit functional goal connection describes an activity. Payers cannot determine medical necessity from an activity description alone. The note needs to answer: why was this activity medically necessary for this specific patient on this specific date? That answer lives in the sentence connecting the activity to the documented functional goal. Our team made this a required field — the note cannot close without it.
Mistake 3 — Separate Time Tracking Not Done for Same-Day Codes
When billing 97110 and 97530 together, each code needs its own time block with separate start and stop times. Estimating total treatment time and splitting it between codes creates documentation that will not survive audit. The exercise block has its own time. The functional activity block has its own time. They do not overlap.
Mistake 4 — No Progression Documentation Across Visits
Payer reviewers looking at multiple 97530 visits expect to see documented evidence that the functional challenge is advancing. Identical activity descriptions across four consecutive visits raise a medical necessity flag. Document a progression element at every session: reduced assistance level, increased task complexity, added dual-task loading, or environmental challenge increase.
Mistake 5 — Documenting Instruction Instead of Active Therapy
97530 requires the patient to be performing the functional activity under direct therapist contact. When the documentation describes the therapist explaining, demonstrating, or reviewing a home program, that describes patient education, not skilled therapeutic activity. If the note reads as instruction rather than active therapy, the code is not supported.
CPT 97530 in Practice — What Our Clinic Actually Does
A patient presents at visit six following left total hip arthroplasty at eight weeks. Hip precautions lifted. Strength testing adequate bilaterally. The remaining gap: she cannot safely perform floor-level tasks — loading the lower dishwasher rack, retrieving items from a low cabinet — because controlled descent to and return from low surfaces has not been practiced under skilled therapeutic guidance.
Our therapist documents the pre-treatment functional status before the session begins: patient unable to perform controlled descent below knee height due to apprehension and asymmetric loading pattern. Functional goal: independent home management including low-surface activities. Clock starts.
The session involves progressive controlled descent to low chair, low stool, and 8-inch surface with manual facilitation at the pelvis, verbal cueing for weight distribution symmetry, and functional task integration — patient retrieves items from a low bin, completes a simulated floor-to-standing sequence, and performs a bilateral overhead-to-low reach pattern reflecting her daily home management demands. Specific cues and patient response are documented at each difficulty level. Outcome: controlled descent to 8-inch surface achieved with supervision, 4-inch surface with minimal assist.
The note closes with the functional goal connection sentence: ‘Low-surface functional task practice targeting patient’s goal of independent home management including floor-level activities following left total hip arthroplasty.’ Total 97530 time: 20 minutes, two units. Documentation written in four minutes. Claim goes out clean.
READY TO STREAMLINE YOUR CLINIC?
See How HelloNote Handles All of This in One Platform
Managing staff hours, compliance, inventory, and financial reports — all inside one HIPAA-compliant EMR built for PT, OT, and SLP clinics.
No credit card required · HIPAA Compliant · PT, OT & SLP
How HelloNote Handles CPT 97530
The HelloNote 97530 template was built around the documentation gap our billing reviews identified most often: functional activity notes that described what happened without establishing why it was a medically necessary skilled service. The template enforces the four required elements as required fields — making correct documentation the default path, not the disciplined one.
- Functional activity description fields — structured inputs for activity name, the functional task being practiced, patient performance level, and multi-outcome components
- Skilled therapist direction field — required section for cues, modifications, and clinical decisions made during the activity
- Start and stop time entry — built into every timed code block with automatic 8-minute rule unit calculation
- Functional goal linkage — required before sign-off, active plan of care goals populate into a selection field
- Same-day code pairing guidance — when 97530 is billed with 97110, HelloNote surfaces documentation guidance so each code has its own justification
- Pre-submission claim scrub — HelloNote checks the 97530 claim against common denial triggers before submission
Frequently Asked Questions About CPT 97530
What does CPT 97530 cover in physical therapy and occupational therapy?
97530 covers functional mobility training (sit-to-stand, transfer training, stair negotiation), ADL task practice (meal preparation simulation, dressing and grooming sequences, home management activities), work simulation for return-to-work clearance, and functional upper extremity tasks in OT. The common thread is multi-outcome functional performance under direct skilled therapist guidance.
What is the 97530 CPT code description?
The official AMA CPT 97530 description is: therapeutic activities, direct one-on-one patient contact by the provider, use of dynamic activities to improve functional performance, each 15 minutes. The activity must be dynamic (patient-performed), functional (resembles real-life tasks), and delivered under direct licensed therapist contact throughout the billed duration.
What are the CPT 97530 billing guidelines for Medicare?
Medicare requires documentation to establish the skilled nature of the service, direct one-on-one therapist contact throughout, and functional medical necessity. The note must identify the specific activity, document the therapist’s skilled direction and clinical decisions, record the patient’s functional performance status, and connect to a documented functional goal. Medicare also requires documented progression across visits.
Can CPT 97110 and 97530 be billed together on the same day?
Yes. Same-day billing is appropriate when each code represents a distinct intervention with separate time tracking and a separate documented clinical justification. 97110 targets the impairment; 97530 practices the functional task that impairment was limiting. Some payers require Modifier 59 — verify payer-specific requirements. Full guide: hellonote.com/97110-vs-97530/
What is Modifier 59 for CPT 97530?
Modifier 59 indicates that two procedures billed on the same day are distinct and separately identifiable services. For 97110 and 97530 billed together, some payers require Modifier 59 to confirm these are not duplicate billings. The modifier signals the separation; the clinical documentation in each note proves it. Never apply Modifier 59 without documentation that clearly establishes the distinct purpose of each code.
How many units of CPT 97530 can I bill per session?
Units are determined by the 8-minute rule: one unit requires at least 8 minutes, two units require at least 23 minutes, three units require at least 38 minutes. Document actual start and stop times, not estimates. When billing 97530 and 97110 together, calculate units for each code from its own separately documented time block.
Is CPT 97530 occupational therapy or physical therapy?
CPT 97530 is used by both occupational therapists and physical therapists. OTs commonly use it for ADL retraining, functional transfer training, and upper extremity task practice. PTs commonly use it for functional gait and transfer training, work simulation, and sport-specific movement practice. The clinical criteria apply identically regardless of discipline.
What triggers an audit or denial for CPT 97530?
Common triggers: high-frequency 97530 billing without documented functional progression, same-day 97110 and 97530 without distinct clinical justifications and separate time documentation, activity descriptions that resemble impairment-level exercise rather than functional task practice, missing functional goal connections, and notes describing therapist instruction rather than patient performance under direct contact.
How does HelloNote help with CPT 97530 billing and documentation?
HelloNote’s 97530 template requires functional activity description with multi-outcome components, skilled therapist direction documentation, start and stop time entry with automatic unit calculation, and functional goal linkage before sign-off. Same-day billing guidance surfaces when 97530 is billed with 97110. Pre-submission claim scrubbing flags missing elements before the claim is submitted.
Start Your Journey to Better CPT 97530 Documentation
The gap between what therapists do in a 97530 session and what ends up in the note is not a clinical gap — it is a documentation habit gap. The clinical work is skilled, complex, and functionally meaningful. The documentation needs to reflect that. Our team built HelloNote to make that reflection automatic, so every 97530 note accurately represents the work and withstands the scrutiny that comes with it.
AboutDmitry Shevchenko, OTR/L
Dmitry Shevchenko, OTR/L is a licensed Occupational Therapist
and the COO of HelloNote EMR. With firsthand experience as both
a practicing clinician and a multi-location clinic operator,
Dmitry brings a unique operational perspective to HelloNote's
product development — having navigated the exact payroll,
compliance, and inventory challenges this platform is built
to solve.