
What is Modifier 59?
Modifier 59 is a CPT modifier used to indicate that two procedures performed on the same day are distinct and separately identifiable services that would not ordinarily be billed together. It tells the payer that each procedure was medically necessary, clinically separate, and performed during a different patient encounter or anatomical site. In physical therapy and occupational therapy, Modifier 59 is most commonly used when billing CPT 97110 and CPT 97530 on the same day. Definition sourced from the Centers for Medicare and Medicaid Services.
Key Takeaways
- Online speech therapy degree programs can be a legitimate pathway when they are properly accredited.
- The professional term is speech-language pathology, but many students search for speech therapy degree programs.
- Online SLP programs usually combine online coursework with supervised clinical practicum requirements.
- Clinical training cannot be completed entirely online because students need supervised patient-facing experience.
- CAA accreditation is one of the most important factors students and employers should verify.
- USAHS is one example of a university offering a hybrid online MS-SLP pathway.
- Clinics should evaluate online SLP graduates based on accreditation, licensure, clinical readiness, communication skills, and documentation ability.
Table of Contents
Modifier 59 is four characters. It appears on a claim in a matter of seconds. And it is responsible for a disproportionate number of billing audits, claim denials, and compliance headaches in outpatient therapy practices across the country. Not because therapists are billing fraudulently — but because Modifier 59 is one of the most misunderstood tools in the billing toolkit, and the consequences of using it incorrectly in either direction are significant.
Use it when you do not need it and you are signaling to a payer that you have intentionally bypassed their bundling edits — which is a compliance flag. Fail to use it when a payer requires it and your same-day claim gets denied or bundled, costing you legitimate revenue. Use it correctly but without documentation that supports it and you are one audit request away from a recoupment demand.
This guide covers what Modifier 59 actually is, when therapy practices need it, how it relates to the X modifiers, what documentation it requires, and the specific mistakes that generate the most audits. For Modifier 59 specific to CPT 97110 and 97530 same-day billing, see our full guide at hellonote.com/97110-vs-97530/

What Is Modifier 59 and Why It Exists
Modifier 59 was created by the Centers for Medicare and Medicaid Services to address a specific billing reality: sometimes two procedures that would normally be bundled together in a single claim are legitimately performed as separate, distinct services on the same day. Without a mechanism to flag this distinction, payers would automatically bundle or deny the second procedure — even when both were clinically appropriate and medically necessary.
The official CMS definition of Modifier 59 is: Distinct Procedural Service. It is used to indicate that the procedure or service was distinct or independent from other non-E/M services performed on the same day. It is applied to a CPT code to tell the payer that this service, while it might appear to overlap with another service billed on the same claim, was in fact performed separately and independently.
Why Payers Bundle Procedures in the First Place
Payers use National Correct Coding Initiative edits — commonly called NCCI edits — to automatically bundle certain CPT code combinations that are typically performed together as part of a single procedure. When two codes appear on the same claim and an NCCI edit exists between them, the payer automatically bundles them and pays only for the higher-value code. Modifier 59 is the mechanism that overrides that bundling when the clinical circumstances genuinely justify billing both codes separately.
The critical word is genuinely. Modifier 59 was not designed as a blanket override for all bundling situations. It was designed for specific clinical circumstances where two procedures that are normally performed together were legitimately performed as separate and distinct services. Using it outside those circumstances — or without documentation that supports the clinical distinction — is a compliance risk regardless of the clinical reality.
When Modifier 59 Is Clinically Justified
Modifier 59 is justified when the two procedures were performed at a different anatomical site, during a different patient encounter on the same day, as separate procedures not ordinarily performed together, or when they represent distinct services with independent clinical justifications that happen to share a bundling edit. In therapy billing, the most common legitimate use is same-day billing of CPT 97110 and CPT 97530 — where each code targets a distinct clinical goal and the two interventions are documented separately with independent medical necessity.
When Do You Need Modifier 59 in Therapy Billing
When should you use Modifier 59 in physical therapy and occupational therapy?
Use Modifier 59 in therapy billing when two CPT codes on the same claim have an NCCI edit between them and the services were genuinely performed as distinct, separately identifiable procedures. The most common therapy scenario is same-day billing of CPT 97110 (therapeutic exercise) and CPT 97530 (therapeutic activity). Not all payers require Modifier 59 — verify requirements per insurer. When required, the documentation must independently justify each code.
Most Common Therapy Scenarios Requiring Modifier 59
CPT 97110 + CPT 97530 on the same day
The most frequent Modifier 59 situation in outpatient PT and OT. Therapeutic exercise targeting a specific impairment (97110) followed by therapeutic activity practicing the functional task that impairment was limiting (97530). Each code needs separate time documentation and separate clinical justification. Some payers require Modifier 59 appended to one of the codes to confirm they are distinct services.
CPT 97110 + CPT 97112 on the same day
Therapeutic exercise for musculoskeletal strengthening (97110) combined with neuromuscular reeducation for proprioceptive deficits (97112). Different clinical targets, different systems treated, same visit. Modifier 59 may be required depending on payer.
CPT 97140 + CPT 97110 on the same day
Manual therapy to restore joint mechanics (97140) followed by therapeutic exercise to build strength through the restored range (97110). Again — distinct clinical purposes, separate documentation required, Modifier 59 may be needed per payer.
Bilateral procedures at different anatomical sites
When the same procedure is performed on two different body regions or anatomical sites in the same session, Modifier 59 (or the more specific XS modifier) documents the separate anatomical sites to justify billing both.
Payer Verification Is Non-Negotiable
Not every payer requires Modifier 59 for the same code combinations. Medicare has specific NCCI edit policies. Commercial insurers have their own bundling rules. Medicaid requirements vary by state. Before appending Modifier 59 to any claim, verify the specific requirement for that payer, that code combination, and that date of service. Applying Modifier 59 when a payer does not require it is not harmful on its own — but it draws attention to the claim. Applying it when a payer requires documentation you do not have is a compliance risk.
Modifier 59 vs XU, XE, XS, XP — The X Modifiers Explained
What is the difference between Modifier 59 and the X modifiers?
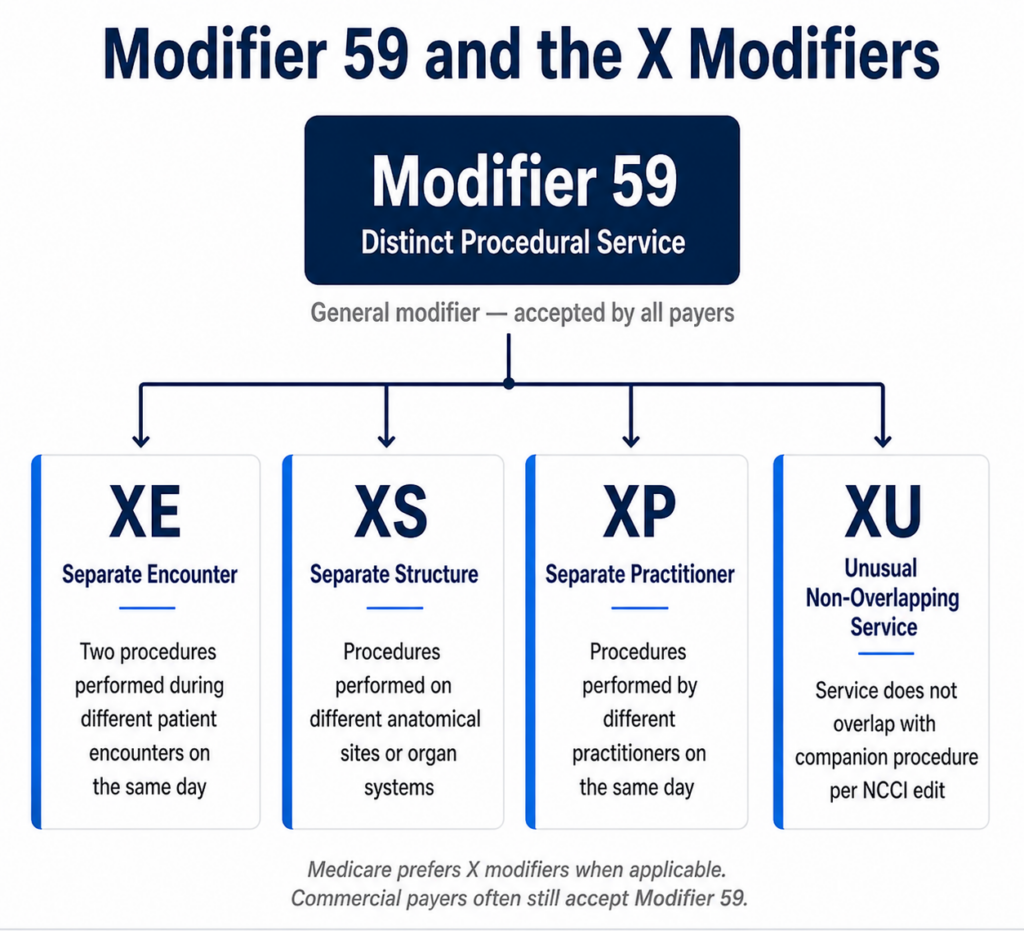
Modifier 59 is the general modifier for distinct procedural services. In 2015 CMS introduced four more specific X modifiers as subsets of Modifier 59: XE (separate encounter), XS (separate structure or anatomical site), XP (separate practitioner), and XU (unusual non-overlapping service). Medicare prefers the X modifiers over Modifier 59 when a more specific modifier applies. Commercial payers vary — many still accept Modifier 59 for all scenarios.
The Four X Modifiers and When Each Applies
XE — Separate Encounter
Use XE when the same procedure was performed twice on the same day but during two completely separate patient encounters — for example, a morning session and an afternoon session. The encounters must be documented separately with distinct start and stop times.
XS — Separate Structure
Use XS when the same procedure was performed on two different anatomical sites or organ systems during the same encounter. Bilateral procedures involving different body regions are the most common therapy application.
XP — Separate Practitioner
Use XP when two different practitioners performed the procedures on the same day. Less common in outpatient therapy but relevant in group practice settings where patients may see more than one clinician in a single day.
XU — Unusual Non-Overlapping Service
Use XU when the service does not overlap with the other procedure as defined by the NCCI edit. This is the closest X modifier to the general use of Modifier 59 and is the one most commonly substituted for Modifier 59 in Medicare claims when a more specific X modifier does not apply.
Which to Use — Modifier 59 or an X Modifier
For Medicare claims, use the most specific X modifier that accurately describes the clinical circumstance. CMS has indicated a preference for the X modifiers over the general Modifier 59 when a specific X modifier applies. For commercial payer claims, check payer-specific guidance — many commercial insurers still accept Modifier 59 for all scenarios and do not require the X modifiers. When in doubt, Modifier 59 is always accepted by Medicare as a fallback when a more specific X modifier is not identified.
NCCI Edits and Modifier 59 — What Therapists Need to Know
National Correct Coding Initiative edits are the bundling rules that determine which CPT code combinations payers automatically bundle when they appear on the same claim. CMS maintains the NCCI edit table and updates it quarterly. Understanding which code pairs have NCCI edits — and whether those edits can be overridden by Modifier 59 — is the foundation of correct Modifier 59 use.
Column One vs Column Two Codes
NCCI edits are organized into column one and column two pairs. The column one code is the comprehensive code — the one that gets paid. The column two code is the component code — the one that gets bundled. When both codes appear on a claim without a modifier, payers pay only the column one code and deny the column two code as included in the comprehensive service.
Some NCCI edits have an indicator of 1, meaning the edit can be overridden with an appropriate modifier like Modifier 59. Others have an indicator of 0, meaning the edit cannot be overridden regardless of modifiers or documentation. This is a critical distinction — applying Modifier 59 to a code pair with an NCCI indicator of 0 will not result in separate payment and may trigger a compliance review.
How to Check NCCI Edits Before Billing
CMS publishes the full NCCI edit table on the CMS website, updated quarterly. Our team recommends checking the NCCI edit table for any new code combination before billing it with Modifier 59 for the first time. The table is searchable by CPT code pair and shows the indicator, the effective date, and the deletion date for each edit. This 60-second check before submitting a claim has prevented more compliance issues in our practice than any other billing habit we have built.
How to Document for Modifier 59
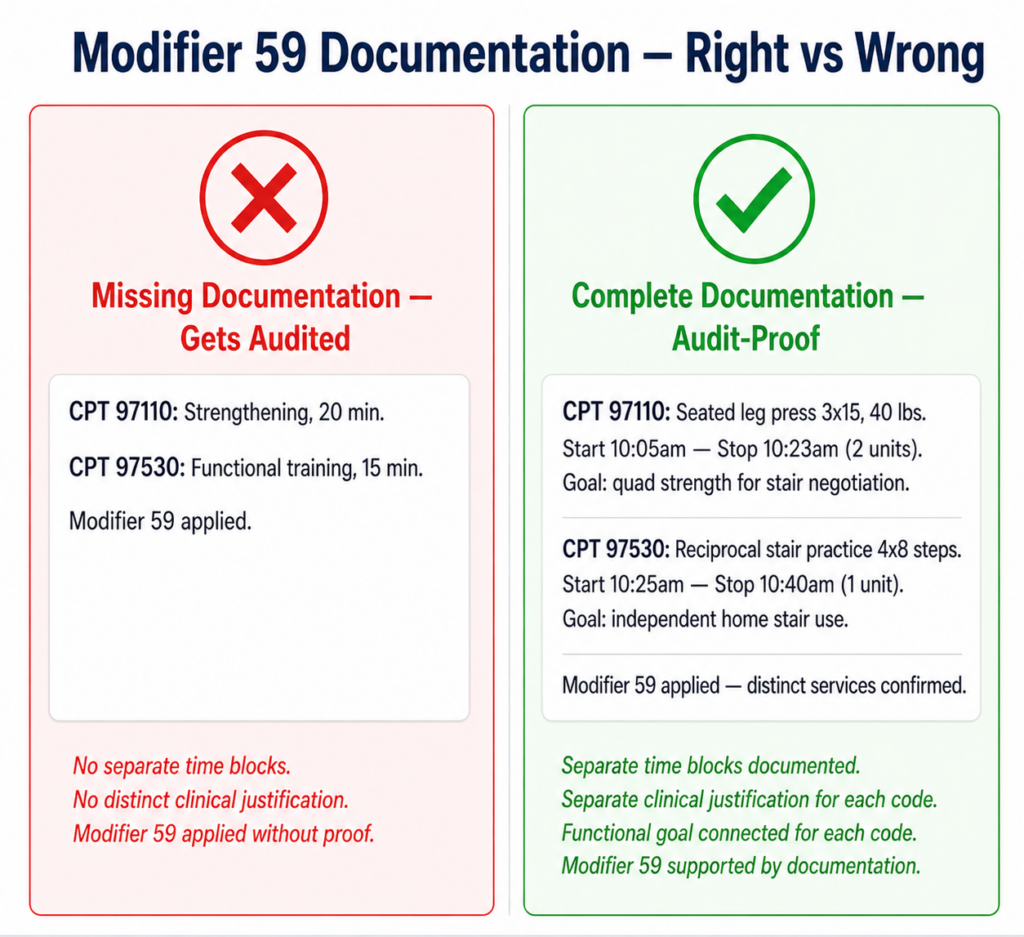
Modifier 59 is only as strong as the documentation behind it. A modifier on a claim is a signal to the payer. The documentation in the note is the proof. When a payer audits a claim with Modifier 59, they are looking at the notes to verify that the two procedures were genuinely distinct, separately performed, and independently medically necessary. If the notes do not show that — the modifier does not save the claim.
The Four Documentation Requirements for Modifier 59 Claims
- Separate time documentation for each code
Each procedure billed on a Modifier 59 claim needs its own start and stop time documented in the note. Not a combined treatment time that gets allocated between codes — actual separate clock times for each distinct service. This is the most fundamental documentation requirement and the most commonly missing element in audited claims.
- Separate clinical justification for each code
Each code needs its own documented clinical rationale establishing the distinct therapeutic purpose of that intervention. The note for CPT 97110 must establish the specific impairment being targeted. The note for CPT 97530 must establish the specific functional task being practiced. A combined description that covers both codes without distinguishing their separate clinical purposes does not support Modifier 59.
- Functional goal connection for each code
Each procedure must be connected to a documented functional goal in the plan of care. This establishes medical necessity independently for each service. When each code has its own functional goal connection, the claim tells a coherent clinical story: we did this (97110) for this reason, and we did that (97530) for this other reason. Both were medically necessary. Both were separate.
- A coherent clinical narrative
The combined documentation across both codes should tell a logical clinical story where the two services are clearly distinct but clinically connected. The impairment addressed in 97110 is the same impairment that was limiting the functional task practiced in 97530. The manual therapy in 97140 restored the mobility that the 97110 exercise then reinforced. When the clinical logic is clear and the documentation reflects it, Modifier 59 claims survive audit.
Common Modifier 59 Mistakes and How to Avoid Them
Mistake 1 — Using Modifier 59 as a Blanket Override
The most dangerous Modifier 59 mistake our team has seen is treating it as a universal fix for any bundled claim. Modifier 59 is not a magic modifier that makes any two codes payable together. It is a specific clinical attestation that two services were genuinely distinct. Applying it routinely to all same-day code combinations without verifying clinical circumstances and NCCI edit indicators is a pattern that triggers compliance reviews. Payers audit modifier usage patterns — a practice that applies Modifier 59 on a high percentage of same-day claims is a red flag.
Mistake 2 — Applying Modifier 59 Without Supporting Documentation
The modifier on the claim and the documentation in the note must align. Applying Modifier 59 without documentation that independently establishes the distinct clinical purpose of each service means the modifier is an assertion without proof. When a payer audits, they will look at the notes. If the notes do not support two separately documented, separately justified, separately timed services — the modifier does not protect the claim. The denial or recoupment follows.
Mistake 3 — Not Verifying Payer Requirements
Not all payers require Modifier 59 for the same code combinations. Not all payers accept the X modifiers. Some commercial payers have their own modifier requirements that differ from Medicare. Our clinic spent time in year two systematically checking modifier requirements for our top five payers by volume and documenting them in our billing reference guide. That 90-minute exercise prevented more denials than any other billing process improvement we made that year.
Mistake 4 — Overriding Non-Bypassable NCCI Edits
NCCI edits with an indicator of 0 cannot be overridden by any modifier. Applying Modifier 59 to these code pairs will not result in separate payment and may trigger a compliance flag. Before billing any code combination with Modifier 59 for the first time, check the NCCI edit indicator. If it is 0, the procedures cannot be billed separately on the same date of service regardless of the clinical circumstances.
Mistake 5 — Combined Time Documentation
Documenting total treatment time and then noting which portion was attributable to each code — rather than documenting separate start and stop times for each code — does not meet the documentation standard for Modifier 59 claims. This approach creates audit risk even when the clinical services were genuinely distinct. Separate time blocks, separately documented, is the only defensible approach.
Modifier 59 in Practice — What Our Clinic Does
Our clinic developed a Modifier 59 protocol in our second year of practice after a commercial payer audit identified a pattern of same-day 97110 and 97530 billing without consistent Modifier 59 documentation. The audit did not result in recoupment — our documentation was adequate — but the experience made us build a process that eliminates the uncertainty entirely.
Every therapist on our team follows the same four-step check before billing any same-day code combination. First, check whether the code pair has an NCCI edit. Second, check whether the edit indicator is 0 or 1. Third, verify whether our primary payer for this patient requires Modifier 59 for this specific code combination. Fourth, confirm that the note includes separate time documentation and separate clinical justification for each code before the claim goes out.
For same-day 97110 and 97530 billing specifically, our HelloNote template handles steps one through four automatically. The system flags the Modifier 59 consideration when both codes appear on the same visit note, requires separate time entry for each code, and will not allow sign-off without functional goal linkage for each code independently. The four-step check happens inside the documentation workflow rather than as a separate billing review step.
The result is that our Modifier 59 claims have a clean submission rate that matches our non-modifier claims. The documentation is correct before the claim goes out. There is nothing to question when a payer reviews it.
READY TO STREAMLINE YOUR CLINIC?
See How HelloNote Handles All of This in One Platform
Managing staff hours, compliance, inventory, and financial reports — all inside one HIPAA-compliant EMR built for PT, OT, and SLP clinics.
No credit card required · HIPAA Compliant · PT, OT & SLP
How HelloNote Handles Modifier 59
When our team built the HelloNote billing workflow, Modifier 59 compliance was one of the specific problems we designed around. The documentation mistakes that generate Modifier 59 audits — combined time tracking, missing clinical justifications, absent functional goal connections — are all structural problems that a well-designed template can prevent at the point of care rather than catch after a denial.
- Modifier 59 flag on same-day code pairs — when CPT codes with common NCCI edits appear on the same visit, HelloNote surfaces a Modifier 59 consideration prompt so the therapist can verify payer requirements before submitting
- Separate time entry per code — each timed code has its own start and stop time field, preventing combined time documentation that does not support Modifier 59 claims
- Separate clinical justification fields — each code requires its own intervention description and clinical rationale before the note can be closed
- Functional goal linkage per code — required before sign-off for each code independently, ensuring medical necessity is documented separately for each service
- Pre-submission claim scrub — flags missing Modifier 59 documentation elements before the claim is submitted so corrections happen before denial rather than after
- Payer-specific modifier guidance — HelloNote surfaces modifier requirements based on the patient’s payer so therapists are not making modifier decisions from memory
The goal was to make correct Modifier 59 billing the path of least resistance — not an additional compliance check at the end of a busy day.
Frequently Asked Questions About Modifier 59
When do you use Modifier 59 in physical therapy?
Use Modifier 59 in physical therapy when two CPT codes on the same claim have an NCCI edit between them, the edit indicator is 1 (bypassable), the services were genuinely performed as distinct procedures, and the payer requires the modifier for that specific code combination. The most common PT scenario is same-day billing of CPT 97110 and CPT 97530. Always verify payer-specific requirements before appending the modifier.
What is the difference between Modifier 59 and Modifier XU?
Modifier 59 is the general distinct procedural service modifier. Modifier XU is one of four X modifiers introduced by CMS in 2015 as more specific subsets of Modifier 59. XU stands for Unusual Non-Overlapping Service and is used when the service does not overlap with the companion procedure as defined by the NCCI edit. Medicare prefers XU (or another X modifier) over Modifier 59 when a specific X modifier accurately describes the clinical circumstance. Commercial payers often still accept Modifier 59 for all scenarios.
Can Modifier 59 be used with CPT 97110 and 97530?
Yes. Modifier 59 is commonly used when CPT 97110 and CPT 97530 are billed on the same day, as some payers require it to confirm these are distinct services rather than duplicate billing. Each code must have separate time documentation, separate clinical justification, and a separate functional goal connection in the note. Verify whether your specific payer requires Modifier 59 for this code combination — not all payers do.
What documentation is required when using Modifier 59?
Modifier 59 documentation requires: separate start and stop times for each code, a separate clinical justification establishing the distinct therapeutic purpose of each service, a separate functional goal connection in the plan of care for each code, and a coherent clinical narrative showing the two services were genuinely distinct. The modifier signals the distinction; the documentation proves it. Missing any of these elements creates audit vulnerability regardless of the modifier.
What are NCCI edits and how do they relate to Modifier 59?
NCCI edits are CMS bundling rules that automatically bundle certain CPT code combinations when they appear on the same claim. Each edit has an indicator: 0 means the edit cannot be overridden by any modifier; 1 means the edit can be overridden with an appropriate modifier like Modifier 59. Before using Modifier 59 on any code pair, check the NCCI edit indicator. Applying Modifier 59 to a code pair with an indicator of 0 will not result in separate payment and may trigger a compliance flag.
What triggers a Modifier 59 audit?
Common Modifier 59 audit triggers include: high-frequency use of Modifier 59 across a large percentage of same-day claims, applying Modifier 59 to code pairs with NCCI indicator 0, claims where the notes do not independently document the distinct clinical purpose of each code, combined time documentation that does not separately support each code, and patterns of Modifier 59 use that do not align with the payer’s modifier policy for specific code combinations.
Do all payers require Modifier 59 for same-day 97110 and 97530?
No. Medicare has specific NCCI edit policies for this code combination. Commercial payers have their own bundling rules and modifier requirements that vary by insurer. Some commercial payers do not require Modifier 59 for 97110 and 97530 billed on the same day. Verify requirements with each payer individually. Applying Modifier 59 when not required is not harmful but may draw unnecessary attention to the claim.
Is Modifier 59 the same as the XS modifier?
No. XS (Separate Structure) is one of four X modifiers that are more specific subsets of Modifier 59. XS applies specifically when two procedures were performed on two different anatomical sites or organ systems. Modifier 59 is the general modifier that applies to any distinct procedural service situation. Use XS when the procedures were genuinely performed on different anatomical structures. Use Modifier 59 or XU when the distinction is based on separate clinical purpose rather than separate anatomical site.
How does HelloNote help with Modifier 59 compliance?
HelloNote flags Modifier 59 considerations when same-day codes with common NCCI edits appear on the same visit. The platform requires separate time entry for each code, separate clinical justification fields, and separate functional goal linkage before sign-off. The pre-submission claim scrub checks for missing Modifier 59 documentation elements before the claim is submitted. Payer-specific modifier guidance surfaces based on the patient’s insurance so modifier decisions are informed, not guessed.
Use Modifier 59 Right — Every Time
Modifier 59 is not complicated when you understand what it is for. It is a clinical attestation — a signal that two services were genuinely distinct and separately performed. The documentation is what makes that attestation defensible. When the documentation is correct, Modifier 59 protects your revenue. When it is not, the modifier creates more audit exposure than billing the codes without it would have. Our team built HelloNote to make correct Modifier 59 documentation the automatic outcome of every same-day billing session — not an afterthought.
Looking up more cpt codes?
See 97110, 97530, and 50+ therapy procedure codes – with billing guidance and documentation tips in one place.
AboutDmitry Shevchenko, OTR/L
Dmitry Shevchenko, OTR/L is a licensed Occupational Therapist
and the COO of HelloNote EMR. With firsthand experience as both
a practicing clinician and a multi-location clinic operator,
Dmitry brings a unique operational perspective to HelloNote's
product development — having navigated the exact payroll,
compliance, and inventory challenges this platform is built
to solve.