

97110 vs 97530: How to Choose the Right CPT Code for Therapy Billing
CPT 97110 vs 97530 — What is the difference?
CPT 97110 is for therapeutic exercise targeting a single musculoskeletal impairment — strength, endurance, range of motion, or flexibility — billed in 15-minute units. CPT 97530 is for therapeutic activities that are functional, multi-outcome, and simulate real-life tasks — also billed in 15-minute units. 97110 changes a tissue capacity. 97530 changes what the patient can do. Both can be billed on the same day when each has separate time tracking and a distinct documented clinical justification.
Key Takeaways
- 97110 targets a single musculoskeletal impairment through isolated therapeutic exercise — 97530 targets functional performance through multi-outcome activities that simulate daily life
- The clinical test is simple: if the intervention changes a tissue capacity, bill 97110 — if it changes what the patient can do, bill 97530
- Both codes can be billed on the same day and often should be — but each needs its own time tracking and its own documented clinical justification
- Modifier 59 may be required by some payers for same-day 97110 and 97530 billing — verify per payer before submitting
- HelloNote’s templates enforce separate clinical justifications for each code so same-day billing is always documented correctly
Table of Contents
Every therapist knows these two codes. Every therapist has questioned them at some point. 97110 and 97530 sit at the center of outpatient PT and OT billing, they often appear on the same claim, and they are the source of more documentation confusion — and more claim denials — than almost any other code pair in the therapy billing system.
The distinction between them is not complicated once you understand it. But understanding it in theory and applying it correctly in a busy clinic with back-to-back patients are two different things. The pressure to chart quickly, the habit of defaulting to familiar codes, the instinct to describe what you did rather than why you did it — these are the conditions that produce billing patterns payers flag and auditors investigate.
This guide is the practical version of the 97110 vs 97530 conversation — the one that covers the clinical distinction, the documentation requirements, the same-day billing rules, and the specific mistakes that generate denials. For the full individual code guides see: hellonote.com/cpt-97110/ and hellonote.com/therapeutic-activity-cpt-code-97530/

CPT 97110 vs 97530 — The Core Clinical Distinction
The distinction between 97110 and 97530 is not about the activity. It is about the clinical target. Two therapists can run their patients through exercises that look nearly identical from across the gym. One is billing 97110 correctly. The other is billing 97530 correctly. The difference is not visible in the room — it is documented in the note.
97110 targets a musculoskeletal impairment. The clinical question is: what specific tissue capacity are we trying to change? Strength, endurance, range of motion, or flexibility — one of those four, targeted directly through therapeutic exercise. 97530 targets a functional performance deficit. The clinical question is: what specific task can the patient not perform, and how do we practice and improve that performance? The answer is always a functional activity — something that resembles what the patient needs to do in their daily life.
The One Question That Resolves Every Code Selection Decision
When our team is deciding between 97110 and 97530, we ask one question: if this intervention worked perfectly, what would be different? If the answer is a tissue measurement — the quad tests at 5/5, the shoulder reaches 150 degrees of flexion, grip strength is 45 pounds — that is 97110. If the answer is a functional task — the patient can get off the floor, climb the stairs to their bedroom, return to their construction job, prepare their own meals — that is 97530. Document the answer to that question. That is your code justification and your medical necessity statement in one sentence.
What is CPT 97110?
What is CPT 97110 (Therapeutic Exercise)?
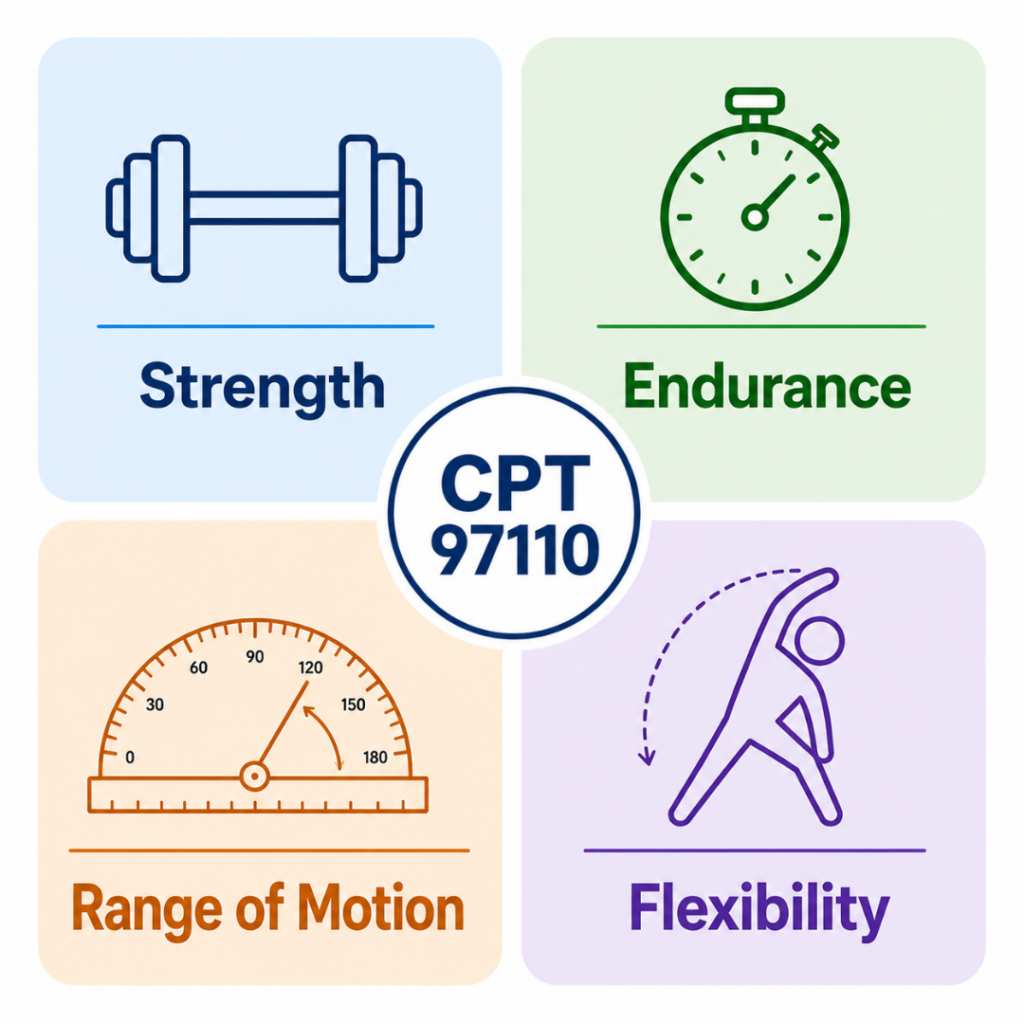
CPT 97110 is a timed therapeutic procedure code for therapeutic exercise targeting a single measurable outcome — strength, endurance, range of motion, or flexibility. Billed in 15-minute units, it requires direct one-on-one licensed therapist contact throughout. It applies when the clinical goal is improving a specific musculoskeletal impairment, not a functional performance deficit. Definition sourced from the American Medical Association CPT code set.
The Four Qualifying Outcomes for 97110
Strength Progressive resistance exercise targeting a specific muscle group or movement pattern with a documented baseline deficit and measurable strength target. MMT grade, dynamometer reading, or pounds of force. Endurance Exercise targeting the ability to sustain a muscle contraction or movement pattern over time, tied to a specific activity demand the patient needs to return to. Range of Motion Structured exercise specifically intended to increase joint or soft tissue mobility, with documented goniometric baseline and target degrees. Flexibility Elongation exercises targeting shortened tissue with documented limitation and functional impact. Outcome measured in degrees or functional reach distance. |
What 97110 Does Not Cover
97110 does not apply to multi-outcome functional activities (use 97530), gait training (use 97116), neuromuscular reeducation targeting proprioceptive or motor control deficits (use 97112), or any exercise performed without continuous direct therapist contact. The code requires a single measurable target and active therapist involvement throughout.
What Is CPT 97530
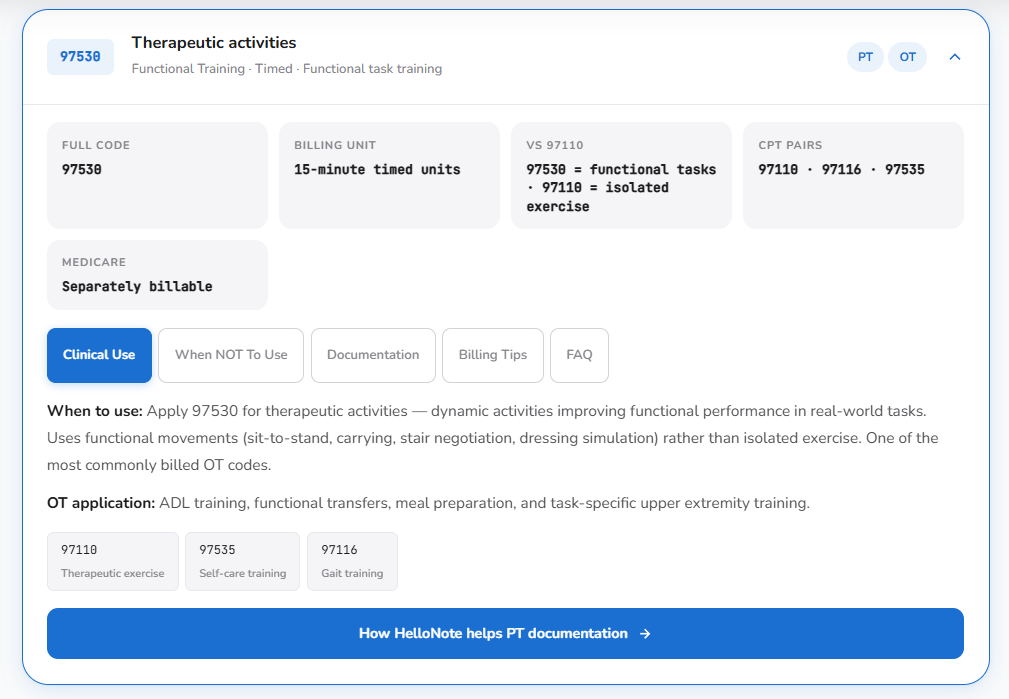
What is CPT 97530 (Therapeutic Activity)?
CPT 97530 is a timed therapeutic procedure code for therapeutic activities — dynamic, functional tasks that simulate real-life activities of daily life. Billed in 15-minute units, it requires direct one-on-one licensed therapist contact throughout. It applies when the clinical goal is improving functional performance through multi-outcome activities, not an isolated musculoskeletal impairment. Definition sourced from the American Medical Association CPT code set.
The Three Clinical Requirements for 97530
Dynamic
The patient is actively performing movement — not being moved by the therapist. The activity requires patient effort and coordination across multiple systems simultaneously.
Functional
The activity mirrors something the patient needs to do in their real life — a task with the multi-joint, multi-outcome complexity of daily living. Not an isolated exercise targeting a single tissue.
Direct
The licensed therapist must be present and actively directing the activity for the entire billed duration. Not supervising from across the room. Direct contact, direct instruction, direct skilled input throughout.
What 97530 Does Not Cover
97530 does not apply to isolated therapeutic exercise targeting a single tissue capacity (use 97110), standalone gait training (use 97116), patient education where the therapist explains or demonstrates rather than directly guiding active patient performance, or any activity performed without continuous direct therapist contact throughout the billed duration.
Side-by-Side Comparison: CPT 97110 vs 97530
| CPT 97110 — Therapeutic Exercise | CPT 97530 — Therapeutic Activity |
|---|---|
| Target: Single musculoskeletal impairment | Target: Functional performance deficit |
| System: Contractile tissue, joint mechanics | System: Functional movement system |
| Outcome: MMT grade, degrees ROM, pounds force | Outcome: Functional task performance |
| Activity: Isolated exercise, single outcome | Activity: Dynamic multi-outcome functional task |
| Patient role: Performs the exercise | Patient role: Performs the functional task |
| Billing unit: 15-minute timed units | Billing unit: 15-minute timed units |
| Direct contact: Required throughout | Direct contact: Required throughout |
| Example: Seated shoulder ER with resistance band | Example: Overhead reaching practice for kitchen tasks |
| Documentation: Functional goal connection sentence required | Documentation: Functional goal connection sentence required |
| Same-day billing: Yes — with 97530 | Same-day billing: Yes — with 97110 |
| Modifier 59: May be required by payer | Modifier 59: May be required by payer |
When to Bill 97110 and 97530 on the Same Day
Billing 97110 and 97530 together on the same day is not just acceptable — it is often the most clinically accurate way to represent a complete outpatient rehabilitation session. The sequence makes clinical sense: therapeutic exercise addresses the specific impairment (97110), then therapeutic activity practices the functional task that impairment was limiting (97530). Build the quad. Practice the stairs. Restore shoulder ROM. Practice the overhead reach. The two codes work as a clinical pair.
The Three Requirements for Defensible Same-Day Billing
- Separate time blocks for each code
Each code needs its own start and stop time documented separately. The exercise block has its own time. The functional activity block has its own time. They do not overlap. Total timed minutes for each code independently satisfies the 8-minute rule.
- Separate clinical justification for each code
The note for 97110 must establish the specific impairment being targeted. The note for 97530 must establish the specific functional task being practiced. Each code needs its own medical necessity statement. Combined or vague documentation that covers both codes with one description is not defensible.
- A coherent clinical narrative connecting both codes
The combined documentation should tell a logical clinical story: we built this capacity (97110) so the patient could practice this functional task (97530). The impairment addressed under 97110 is the same impairment that was limiting the functional task practiced under 97530. When this connection is clear in the note, same-day billing is not an audit flag — it is complete documentation.
Modifier 59 for CPT 97110 and 97530
When do you need Modifier 59 for CPT 97110 and 97530?
Modifier 59 is required by some payers when CPT 97110 and 97530 are billed on the same day to confirm they represent distinct and separately identifiable services. Not all payers require it — verify requirements per insurer before submitting. When required, the documentation must provide the clinical distinction the modifier signals: the modifier tells the payer these are separate services; the notes prove it.
Modifier 59 does not protect a poorly documented claim. It signals to the payer that two codes on the same claim represent separate procedures — but if the clinical notes do not clearly establish the distinct purpose of each code, the modifier alone will not prevent a denial or audit. The modifier and the documentation work together. Never apply Modifier 59 without documentation that independently justifies each code.
Documentation Requirements for Each Code
What Every 97110 Note Must Include
- Specific exercise name and description — not ‘strengthening exercises’ but ‘seated resisted shoulder external rotation, 3 x 12, 3 lb, pain-free arc 0–90 degrees’
- Exercise parameters — sets, repetitions, resistance or load, patient position
- Actual start and stop time — not an estimate, the real clock times
- Objective outcome measure — the session’s result compared to baseline
- Functional goal connection sentence — the one sentence connecting the impairment-level work to a functional goal in the plan of care
What Every 97530 Note Must Include
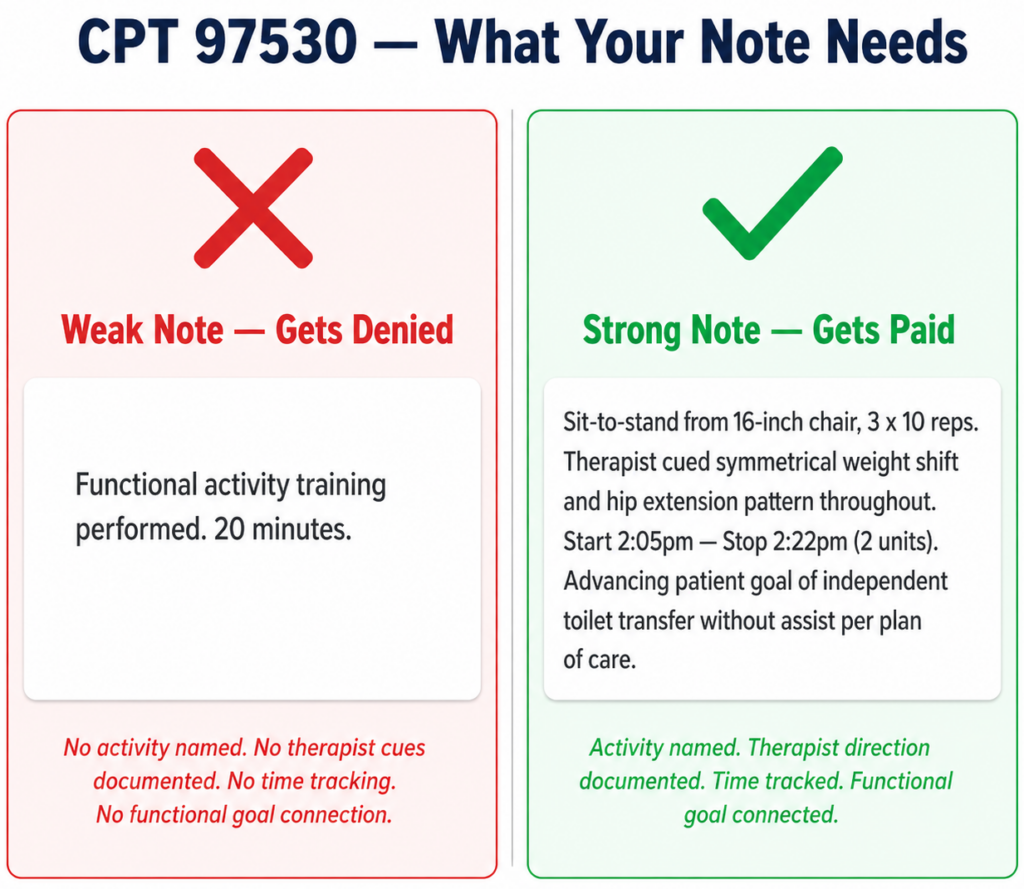
- Specific activity name and its multi-outcome components — not ‘functional activity training’ but ‘reciprocal stair negotiation, 3 x 8 steps, targeting loading tolerance, dynamic balance, and hip extension mechanics’
- Skilled therapist direction throughout — specific cues provided, modifications made, clinical decisions during the activity
- Actual start and stop time — separate from the 97110 time block
- Functional goal connection sentence — connecting the activity to the documented functional goal in the plan of care
Common Coding Mistakes and How to Avoid Them
Mistake 1 — Using 97530 for Impairment-Level Exercise
Applying 97530 to exercises that are genuinely 97110 interventions because they happen in a functional position or involve multiple joints. A standing exercise is not automatically a functional activity. Code to the clinical intent: if the therapeutic goal is a tissue capacity, the code is 97110 regardless of the exercise position or the number of joints involved.
Mistake 2 — Using 97110 for Multi-Outcome Functional Activities
Defaulting to 97110 for activities that involve multiple simultaneous clinical outcomes and resemble daily life tasks. Sit-to-stand practice, stair negotiation, kitchen simulation, and work task replication are 97530 activities regardless of the strength component involved. If the activity is functional and multi-outcome, the code is 97530.
Mistake 3 — Combined Time Documentation for Same-Day Codes
Estimating total treatment time and splitting it between 97110 and 97530 without separate documented time blocks. Each code needs its own start and stop time. When payers audit same-day billing, separate time documentation is the first thing they verify. If it is not there, the claim is vulnerable regardless of how appropriate the clinical interventions were.
Mistake 4 — Missing the Functional Goal Connection on Both Codes
Documenting the exercise or activity accurately while omitting the sentence that connects it to a functional goal in the plan of care. This is the most common denial reason for both codes. Medical necessity is not established by describing the intervention — it is established by connecting the intervention to a documented functional outcome that justifies why the patient needs skilled therapy to achieve it.
Mistake 5 — Applying Modifier 59 Without Supporting Documentation
Using Modifier 59 on same-day 97110 and 97530 claims without documentation that independently justifies each code. Modifier 59 signals separate services — the notes prove it. If both codes share a single combined description in the note, Modifier 59 will not prevent a denial.
CPT 97110 vs 97530 in Practice — What Our Clinic Does
A patient presents at visit four following right knee arthroplasty. Assessment this session: quadriceps strength 3+/5 right versus 5/5 left, active knee extension lacking 15 degrees compared to the uninvolved side, and single-leg stance time 8 seconds right versus 22 seconds left. The patient’s documented goal is returning to independent stair use in his two-story home within six weeks.
Our team’s session plan: therapeutic exercise first targeting the quad strength and knee extension deficit (97110), followed by therapeutic activity practicing the stair negotiation pattern the patient needs to achieve his functional goal (97530).
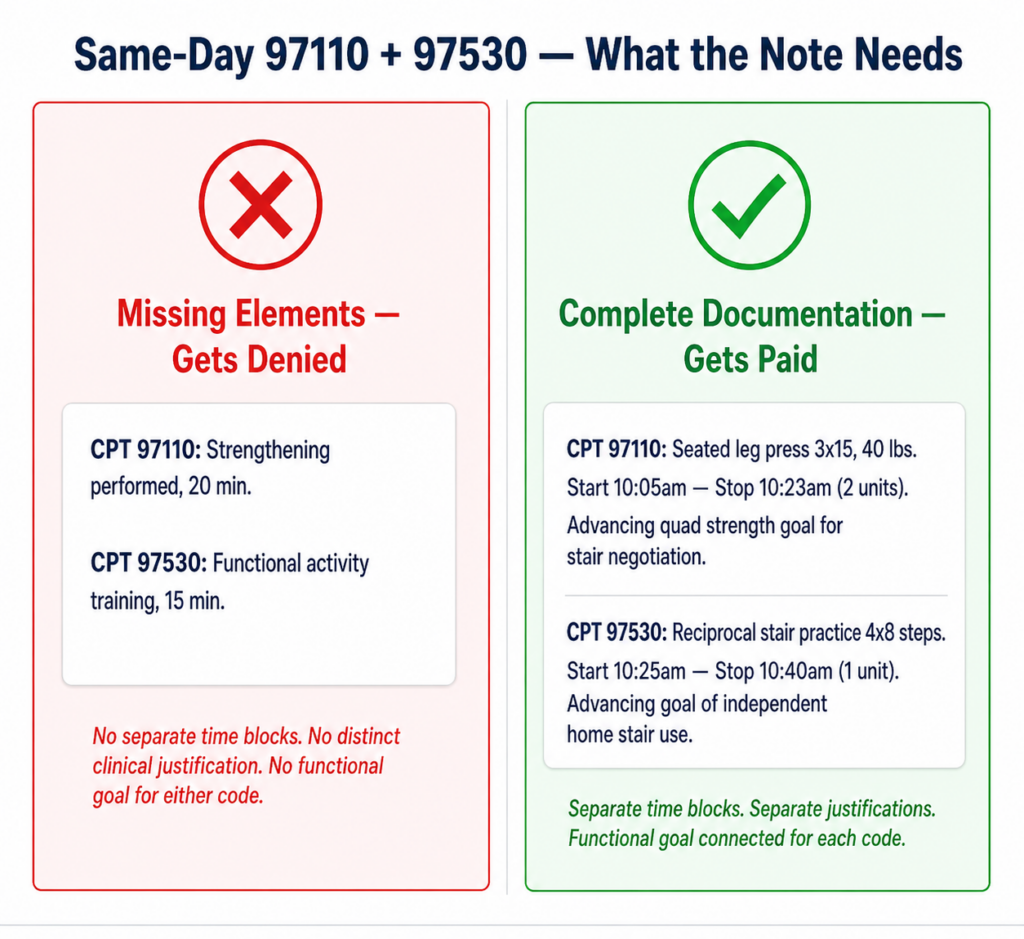
The 97110 block runs 18 minutes: seated leg press 3 x 15 at 40 lbs targeting knee extension strength, terminal knee extensions 3 x 20 with theraband targeting quad recruitment in terminal range. Start time 10:05am, stop time 10:23am. Two units. Note documents the specific exercises, parameters, resistance, and the outcome measure: active knee extension improved from −15 to −10 degrees by end of session. Functional goal connection: ‘Quad strengthening targeting 5/5 strength required for safe reciprocal stair negotiation per patient’s goal of independent stair use in his home.’
The 97530 block runs 15 minutes: reciprocal stair negotiation on 4-step training stairs, 4 sets ascending and descending, with therapist cuing weight distribution symmetry and controlled knee flexion loading on descent. Start time 10:25am, stop time 10:40am. One unit. Note documents the activity, cues provided, patient response, and the functional goal connection: ‘Stair negotiation practice advancing patient’s goal of independent two-story home stair use without handrail assist.’
Two codes. Separate time blocks. Separate clinical justifications. A coherent clinical story where the 97110 impairment work directly supports the 97530 functional task practice. This is same-day billing done correctly.
READY TO STREAMLINE YOUR CLINIC?
See How HelloNote Handles All of This in One Platform
Managing staff hours, compliance, inventory, and financial reports — all inside one HIPAA-compliant EMR built for PT, OT, and SLP clinics.
No credit card required · HIPAA Compliant · PT, OT & SLP
How HelloNote Handles CPT 97110 and 97530
When our team built the HelloNote documentation templates, the 97110 vs 97530 distinction drove several core design decisions. The two most important: each code has its own separate time entry field, and each code requires its own functional goal linkage before the note can be closed. These two structural requirements eliminate the most common same-day billing mistakes before the claim is ever submitted.
- Separate time entry per code — start and stop times are entered independently for each timed code block. HelloNote calculates units for each code separately using the 8-minute rule. There is no combined time field that gets split between codes.
- Separate functional goal linkage — each code must be connected to a plan of care goal before sign-off. The 97110 goal and the 97530 goal are documented independently. The note cannot close until both connections are made.
- Same-day code pairing guidance — when 97110 and 97530 appear on the same visit, HelloNote surfaces documentation guidance so the clinical distinction between the two codes is captured in the note structure.
- Pre-submission claim scrub — before the claim goes out, HelloNote checks both codes against common denial triggers and flags missing elements for review.
- Modifier 59 reminder — when 97110 and 97530 are billed together, HelloNote flags the Modifier 59 consideration so the therapist can verify payer requirements before submission.
Frequently Asked Questions — CPT 97110 vs 97530
What is the difference between CPT 97110 and CPT 97530?
CPT 97110 is for therapeutic exercise targeting a single musculoskeletal impairment — strength, endurance, range of motion, or flexibility. CPT 97530 is for therapeutic activities that are functional, multi-outcome, and simulate real-life tasks. 97110 changes a tissue capacity. 97530 changes what the patient can do. The distinction is clinical intent, which must be documented explicitly in the note for both codes.
Can you bill CPT 97110 and 97530 on the same day?
Yes. Same-day billing of 97110 and 97530 is appropriate when each code represents a distinct intervention with separate time tracking and a separate documented clinical justification. 97110 addresses the musculoskeletal impairment; 97530 practices the functional task that impairment was limiting. Some payers require Modifier 59 for same-day billing — verify payer-specific requirements before submitting.
When should I use 97110 instead of 97530?
Use 97110 when the therapeutic goal is to change a single tissue capacity: strengthen a specific muscle group, increase ROM in a specific direction, improve endurance for a specific demand, or increase flexibility in shortened tissue. If the intervention targets one measurable impairment through isolated exercise, bill 97110. If the activity is functional, multi-outcome, and resembles a daily life task, bill 97530.
When should I use 97530 instead of 97110?
Use 97530 when the therapeutic goal is to improve a patient’s ability to perform a specific functional task — sit-to-stand, stair negotiation, meal preparation, transfer training, work simulation, sport-specific movement. The activity must be dynamic (patient-performed), functional (resembles real-life tasks), and delivered under direct therapist contact throughout the billed duration.
What is Modifier 59 for 97110 and 97530?
Modifier 59 indicates that two procedures billed on the same day are distinct and separately identifiable services. Some payers require it when 97110 and 97530 are both billed on the same claim to confirm they are not duplicate billings of the same service. The modifier signals separation; the clinical documentation in each note proves it. Never apply Modifier 59 without documentation that clearly establishes the distinct clinical purpose of each code.
How many units of 97110 and 97530 can I bill per session?
Units for each code are determined independently by the 8-minute rule. One unit requires at least 8 minutes of direct therapist contact, two units require at least 23 minutes, three units require at least 38 minutes. Calculate units for 97110 from its own documented time block and units for 97530 from its own separate time block. The total combined time determines neither — each code stands on its own time documentation.
Is CPT 97110 or 97530 used in occupational therapy?
Both codes are used in occupational therapy and physical therapy. OTs commonly bill 97110 for isolated upper extremity strengthening, grip and pinch strengthening, and ROM exercises following hand or shoulder conditions. OTs commonly bill 97530 for ADL retraining, functional upper extremity task practice, home management simulation, and work task replication. The clinical criteria apply identically regardless of discipline.
What triggers an audit for same-day 97110 and 97530 billing?
Common audit triggers include: combined time documentation that gets split between codes rather than separately tracked, notes where both codes share a single clinical description without distinct justifications, high-frequency same-day billing without documented clinical rationale for both codes in every visit, and Modifier 59 applied without supporting documentation that establishes the separate nature of each service.
How does HelloNote help with 97110 and 97530 same-day billing?
HelloNote’s templates require separate time entry and separate functional goal linkage for each code before the note can be closed. Same-day code pairing guidance surfaces when both codes appear on the same visit. The pre-submission claim scrub checks both codes against common denial triggers. Modifier 59 is flagged for payer verification when 97110 and 97530 are billed together.
Bill Both Codes Right — Every Session
The 97110 vs 97530 distinction is not a compliance technicality. It is a clinical documentation practice that accurately represents the work being done and protects the revenue that work generates. When both codes are documented correctly — with separate time blocks, separate clinical justifications, and clear functional goal connections — same-day billing is not a risk. It is an accurate billing record of a complete, skilled rehabilitation session.
Looking up more cpt codes?
See 97110, 97530, and 50+ therapy procedure codes – with billing guidance and documentation tips in one place.