
Table of Contents
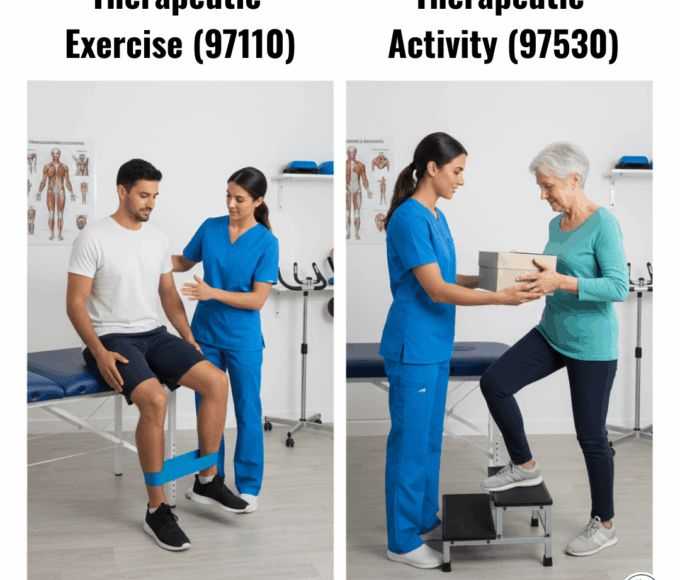
In 2026, the 8-Minute Rule remains the CMS standard for billing timed CPT codes (like 97110 and 97140). To bill one unit, you must provide at least 8 minutes of direct care. For 2026, the Medicare Physician Fee Schedule (MPFS) has finalized a $33.4009 conversion factor (a 3.26% increase from 2025), making accurate unit calculation essential to offset the new -2.5% efficiency adjustment applied to non-timed work RVUs.
Clinical Methodology and 2026 Regulatory Compliance
The financial landscape of 2026 is governed by stricter transparency laws and updated CMS fee structures.
The No Surprises Act and Estimate Accuracy
For every self-pay or out-of-network patient, clinics must provide a Good Faith Estimate (GFE) within one to three business days of scheduling. This document must include expected CPT codes (e.g., 97110, 97140) and diagnostic ICD-10 codes.
Audit Warning: If the final bill exceeds the GFE by $400 or more, patients have a federal right to dispute the charges. Estimate accuracy is no longer just a courtesy—it is a critical compliance metric for 2026.
Mastering the 8-Minute Rule in 2026
The 8-Minute Rule remains the gold standard for Medicare. To bill a single unit of a timed service, a therapist must provide at least 8 minutes of direct, one-on-one care.
In 2026, payers have increased their use of “Supplemental Portion” audits, scrutinizing “mixed remainders”—the leftover minutes from different interventions. HelloNote’s real-time unit calculator prevents these errors by automatically applying the 8-Minute Rule logic as you type your note.
2026 Cost Drivers: Insurance vs. Self-Pay
| Factor | Insurance (In-Network) | Self-Pay / Out-of-Network | HelloNote Integration |
|---|---|---|---|
| Conversion Factor | Fixed at $33.40 (MPFS) | Determined by Clinic | Automated Fee Schedules |
| Price Transparency | EOB (Post-Service) | Good Faith Estimate | Built-in GFE Generator |
| Assistant Modifier | 15% reduction (CO/CQ) | Usually Full Rate | Auto-Modifier Application |
| Complexity Level | 3-Tier Eval (97161–97163) | Flat Evaluation Fee | Complexity-Driven Templates |
The "Therapist’s Insight": Combating Sticker Shock
In my clinical practice, the most dangerous time for patient retention isn’t the first session—it’s the arrival of the first bill. With deductibles often exceeding $3,000 in 2026, a patient might see a $450 bill for their first three visits and immediately cancel.
The Financial Evaluation Strategy
Perform a “Financial Evaluation” simultaneously with your Clinical Evaluation. Use HelloNote’s Insurance Verification tool before the patient walks in. I tell my patients:
“Your plan has a $3,000 deductible, which means today’s session will cost approximately $125. However, completing this 8-week plan now prevents a $20,000 surgery next year.”
By framing the cost as an investment in “Surgery Prevention,” you shift the psychological value from a “bill” to a “saving.”
Frequently Asked Questions
Q1. What is the "Efficiency Tax" on my 2026 claims?
CMS finalized a 2.5% reduction in work Relative Value Units (RVUs) for most non-time-based services (like evaluations). This reflects a federal assumption that “workflow improvements,” such as AI Scribes, have made these tasks faster to complete.
Q2. Can I bill for a 30-minute session if I only spent 22 minutes with the patient?
No. Under the 8-Minute Rule, 22 minutes equals one unit (8–22 mins). You must reach at least 23 minutes of direct care to bill two units.
Q3. Do I need a new Good Faith Estimate if the patient's diagnosis changes?
Yes. If the scope of care changes significantly (e.g., a patient with LBP develops sciatica), you must issue an updated GFE at least one business day before the next session.
Q4. What is the 2026 KX Modifier threshold?
For 2026, the KX modifier threshold is $2,480 for PT and SLP combined, and $2,480 for OT.
Q5. Does the 15% assistant reduction apply to all codes?
No. It only applies to the practice expense (PE) portion of the payment for services billed with the CO or CQ modifiers when a PTA or OTA provides more than 10% of the service.