AI Scribe for Physical Therapists: Beyond Saving Time
What Are the Real Benefits of AI Scribe for Therapists?
The biggest benefits of AI scribe for therapists are improved clinical presence, more complete documentation, reduced cognitive fatigue, fewer after-hours notes, and better billing accuracy. Instead of reconstructing sessions from memory at the end of the day, AI scribe captures the clinical encounter in real time so therapists can stay focused on the patient while generating more consistent documentation.
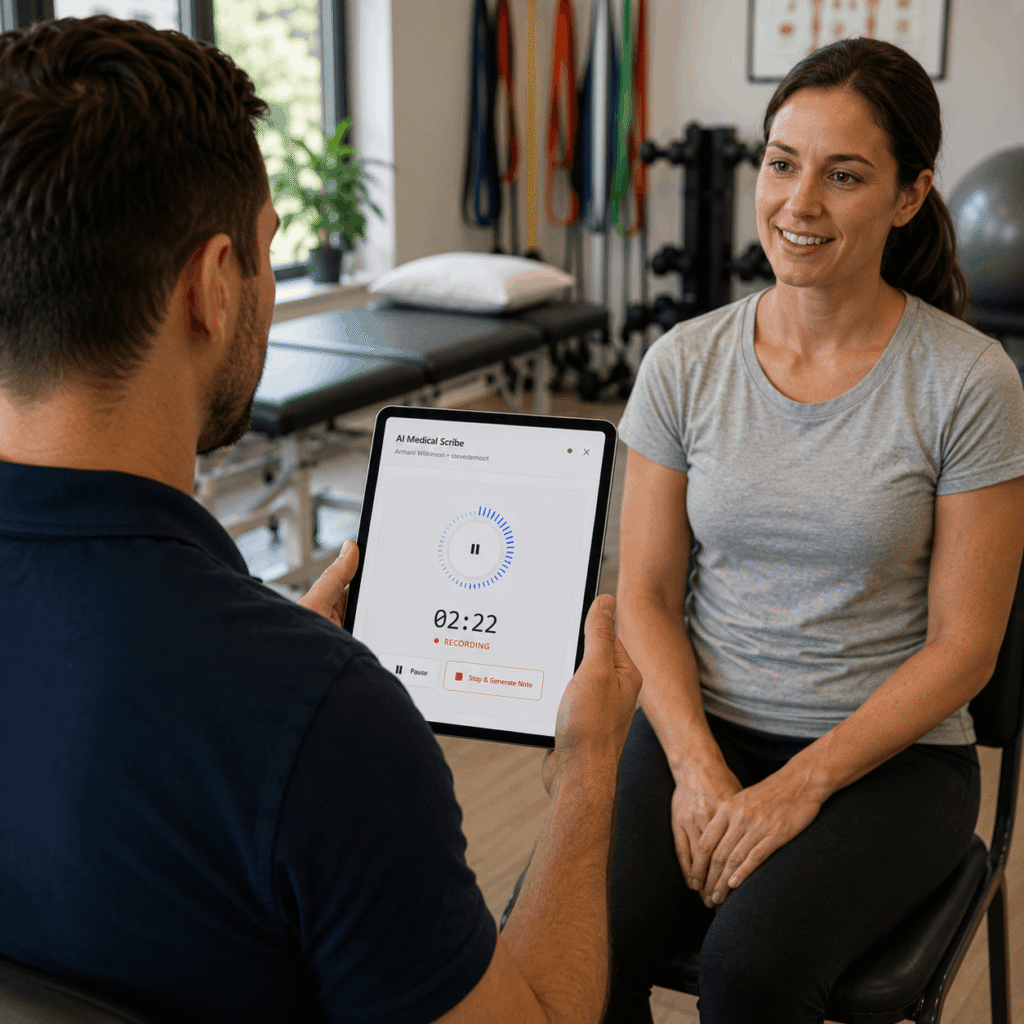
Table of Contents
Key Takeaways
- The most underreported benefit of AI scribe is not speed – it is the return of full clinical presence during patient sessions.
- Therapists using AI scribe report lower end-of-day cognitive fatigue, not just shorter charting sessions – the mental load of parallel documentation tracking disappears.
- HelloNote AI Scribe gives clinicians the specific benefit of context-aware drafts – the note already knows the patient, the case, and the payer before the session starts.
What Clinicians Actually Lose Every Day Before AI Scribe
We want to start this post differently than every other AI scribe benefits article you have read. Not with what therapists gain. With what they lose.
We had a patient a few years back – bilateral shoulder dysfunction, complex history, a lot of layers to track. Midway through the evaluation, while she was explaining how her symptoms had changed since her last flare, our therapist caught herself doing something she had trained herself not to do: mentally filing details for the note instead of fully listening to the patient. Onset timeline. Bilateral vs unilateral presentation. The exact phrase the patient used about reaching across her body. Two tracks running simultaneously – one clinical, one documentary. The patient was still talking. Our therapist was still nodding. But part of her attention had already left the room.
That split is so normalized in therapy practice that most clinicians do not notice it anymore. It is just how documentation works. You treat and you file. You listen and you catalog. You stay present and you prepare the reconstruction. And at the end of the day, when the last patient has left and the notes still need to be finished, you find out how much of that mental filing actually held.
AI scribe does not just save documentation time. It closes the split. And everything that follows in this post is a consequence of that one change.
The Presence Benefit - Being Fully in the Room
Clinical presence – the quality of being fully attentive and engaged with the patient – is not just a therapeutic nice-to-have. It is a clinical instrument. A therapist who is fully present catches the wince the patient tries to suppress. Hears the hesitation before they describe their pain level. Notices the compensatory movement pattern that only appears when the patient forgets they are being observed. These are diagnostic signals that a divided attention misses.
The Parallel Processing Tax
Every experienced therapist has developed some version of parallel processing – the ability to treat and mentally document simultaneously. It is a skill born of necessity, not preference. And like all divided attention states, it has a cost. The cost is paid in clinical granularity – the small observations that fall through the gap between the track that is treating and the track that is filing.
When AI scribe takes over the documentation track entirely, clinicians consistently report noticing more during sessions. Not because their clinical skills improved. Because the cognitive bandwidth that was split between treating and documenting is now fully allocated to treating. That is the presence benefit, and it shows up in note quality, patient rapport, and clinical outcome in ways that are hard to quantify but easy to recognize once you have experienced it.
What Patients Notice Too
Patients are perceptive. A therapist who is writing between patient responses, mentally composing sentences while asking the next question, or glancing at a template while listening to a symptom description communicates something about the quality of attention in the room. Patients may not name it, but they feel it. AI scribe removes the competing demand on the clinician’s attention so that the patient gets the version of their therapist who is entirely there.
Looking for cpt and icd codes guide?
See 97110, 97530, and 50+ therapy procedure codes – with billing guidance and documentation tips in one place.
The Quality Benefit - Notes Written From the Session, Not From Memory
Documentation quality in therapy is not just about compliance – it is about clinical communication, audit protection, and the continuity of care across providers and payers. A note written from memory two hours after a session is structurally different from a note generated from the actual session conversation. Both can be accurate. But they are not equally complete.
Memory Is Selective. Transcripts Are Not.
Human memory prioritizes significance. When a therapist reconstructs a session from memory, they document what stood out – the measurable findings, the primary complaints, the clinical decisions. What frequently gets compressed or omitted is the clinical context: the specific language the patient used, the sequence in which symptoms were reported, the observation that was noted but not immediately acted on. These details matter in an audit. They matter when a different clinician sees the patient. They matter when a payer reviewer is deciding whether continued treatment is medically necessary.
Consistency Across the Caseload
Documentation quality in manual charting is inversely correlated with patient volume and end-of-day fatigue. The tenth note of the day is almost always less complete than the first. AI scribe removes that variable. Every session generates a transcript of equal completeness. Every draft note starts from the same quality of source material regardless of whether the patient was seen at 8am or 5pm. For practices trying to maintain documentation standards across a busy caseload, that consistency is a meaningful clinical benefit.
The Burnout Benefit - Removing the Hidden Cognitive Load
Clinician burnout in therapy is well-documented. What is less well-understood is the specific mechanism by which documentation contributes to it. It is not simply the hours spent charting – though those matter. It is the sustained dual-processing demand that documentation imposes across an entire clinical day.
The Cognitive Cost of Parallel Documentation Tracking
Every session a therapist conducts without AI scribe involves some degree of parallel cognitive processing – treating in the foreground, filing for documentation in the background. By the end of a ten-patient day, the therapist has not only treated ten patients. They have also maintained ten parallel documentation tracks simultaneously, each requiring active mental management throughout the session and reconstruction afterward. That sustained load is a significant contributor to the end-of-day exhaustion that precedes burnout.
A 2025 UCLA Health study found that AI scribe use was associated with meaningful reductions in clinician burnout scores. The mechanism is not mysterious: when the documentation track is handled by the AI, the mental load of the clinical day decreases even when the patient volume stays the same. Therapists who have used AI scribe consistently report feeling less depleted at the end of the day – not because they treated fewer patients, but because each session required less of them cognitively.
Getting the Evening Back
After-hours documentation is one of the most cited contributors to therapy burnout. A therapist who finishes clinic at 5pm and spends until 7pm finishing notes has not had a workday that ended at 5pm. AI scribe does not just compress the documentation time within clinic hours. For many practices, it eliminates the after-hours documentation requirement entirely. The note that used to be written at 9pm on the couch is now a reviewed and finalized draft by 5:15.
The Billing Accuracy Benefit - Capturing What Actually Happened
Documentation accuracy has a direct financial dimension that is easy to underestimate. Undertimed units, missing laterality, vague functional goal language, and unsupported skilled care rationale are all documentation quality failures that cost practices money – either through claim denials, audit repayments, or the silent revenue loss of consistent underbilling.
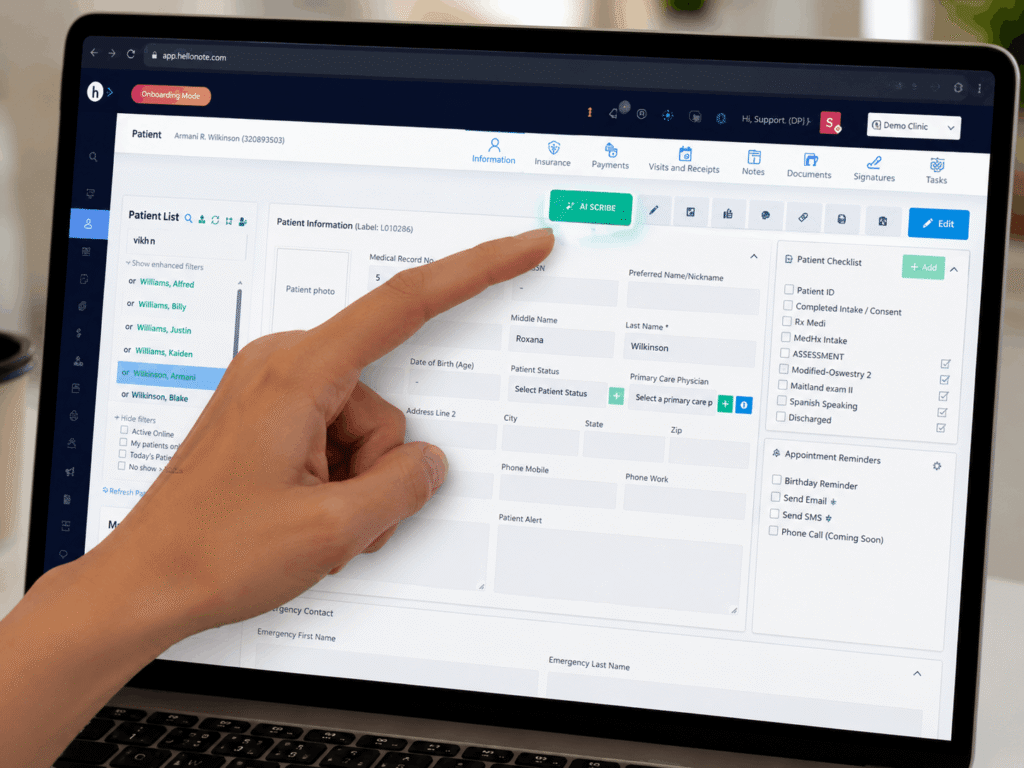
AI scribe captures session time in real time. It captures the specific interventions as they are described during the session. It captures the clinical reasoning the therapist articulates out loud. When that captured content is used to generate the draft note, the documentation reflects what actually happened with a fidelity that manual post-session charting rarely achieves consistently. For practices using HelloNote AI Scribe with integrated CPT code suggestions, the billing accuracy benefit extends to code selection – with the AI reading the drafted note and suggesting the most appropriate codes based on what was documented.
How HelloNote AI Scribe Delivers These Benefits in Practice
The benefits described in this post are not hypothetical. They are the outcomes of a documentation workflow that starts with the session itself rather than a blank screen. Here is how HelloNote AI Scribe delivers them specifically.
- Full clinical presence – AI Scribe handles documentation capture during the session so the therapist’s full attention stays on the patient, not split between treating and filing.
- Session-accurate drafts – the note is built from a transcript of the actual encounter, not reconstructed from memory, producing more complete and consistent documentation across the entire caseload.
- Reduced end-of-day cognitive load – the parallel documentation tracking that contributes to clinician fatigue across the day is removed from the therapist’s cognitive demand.
- After-hours documentation reduction – draft notes are available for review immediately after the session, eliminating the primary driver of after-hours charting for most practices.
- Billing accuracy support – integrated CPT code suggestions based on documented note content help practices capture all billable units accurately from every session.
READY TO STREAMLINE YOUR CLINIC?
See How HelloNote Handles All of This in One Platform
Managing staff hours, compliance, inventory, and financial reports — all inside one HIPAA-compliant EMR built for PT, OT, and SLP clinics.
No credit card required · HIPAA Compliant · PT, OT & SLP
Frequently Asked Questions About AI Sribe.
What are the main benefits of AI scribe for physical therapists?
The primary benefits of AI scribe for physical therapists are improved clinical presence during sessions, more complete and consistent documentation, reduced end-of-day cognitive fatigue, elimination of after-hours charting, and improved billing accuracy through real-time session capture. The presence benefit - therapists being fully attentive rather than mentally filing for notes - is often reported as the most significant change in clinical practice.
Does AI scribe improve documentation quality or just speed?
Both, but quality improvement is often the more significant benefit. Because AI scribe generates notes from a transcript of the actual session rather than from memory reconstruction, the resulting documentation is typically more complete, more consistent across the caseload, and more accurate in capturing clinical details that would otherwise be compressed or omitted in manual charting.
Can AI scribe help reduce therapist burnout?
Yes. A 2025 UCLA Health study found meaningful reductions in clinician burnout associated with AI scribe use. The mechanism involves removing the sustained cognitive demand of parallel documentation tracking across the clinical day and eliminating the after-hours documentation that is one of the most cited burnout contributors in therapy practice.
How does AI scribe improve billing accuracy for therapy practices?
AI scribe captures session content in real time, including the specific interventions performed, time allocations, and clinical reasoning articulated during the session. This produces documentation that more accurately reflects what happened than manual post-session charting, reducing undertimed units, missing laterality, and vague clinical language that lead to claim denials and audit exposure.
What is the difference between AI scribe benefits for OT vs PT vs SLP?
The core benefits apply across all therapy disciplines, but the clinical presence and documentation quality benefits manifest differently by discipline. For OTs, improved presence means better observation of functional performance and occupational behavior. For PTs, it means more complete capture of movement analysis and functional mobility data. For SLPs, it means more accurate documentation of communication and swallowing observations that are difficult to reconstruct from memory.