
How Long Does Physical Therapy Take to Work? Your 2026 Recovery Timeline Guide
Table of Contents
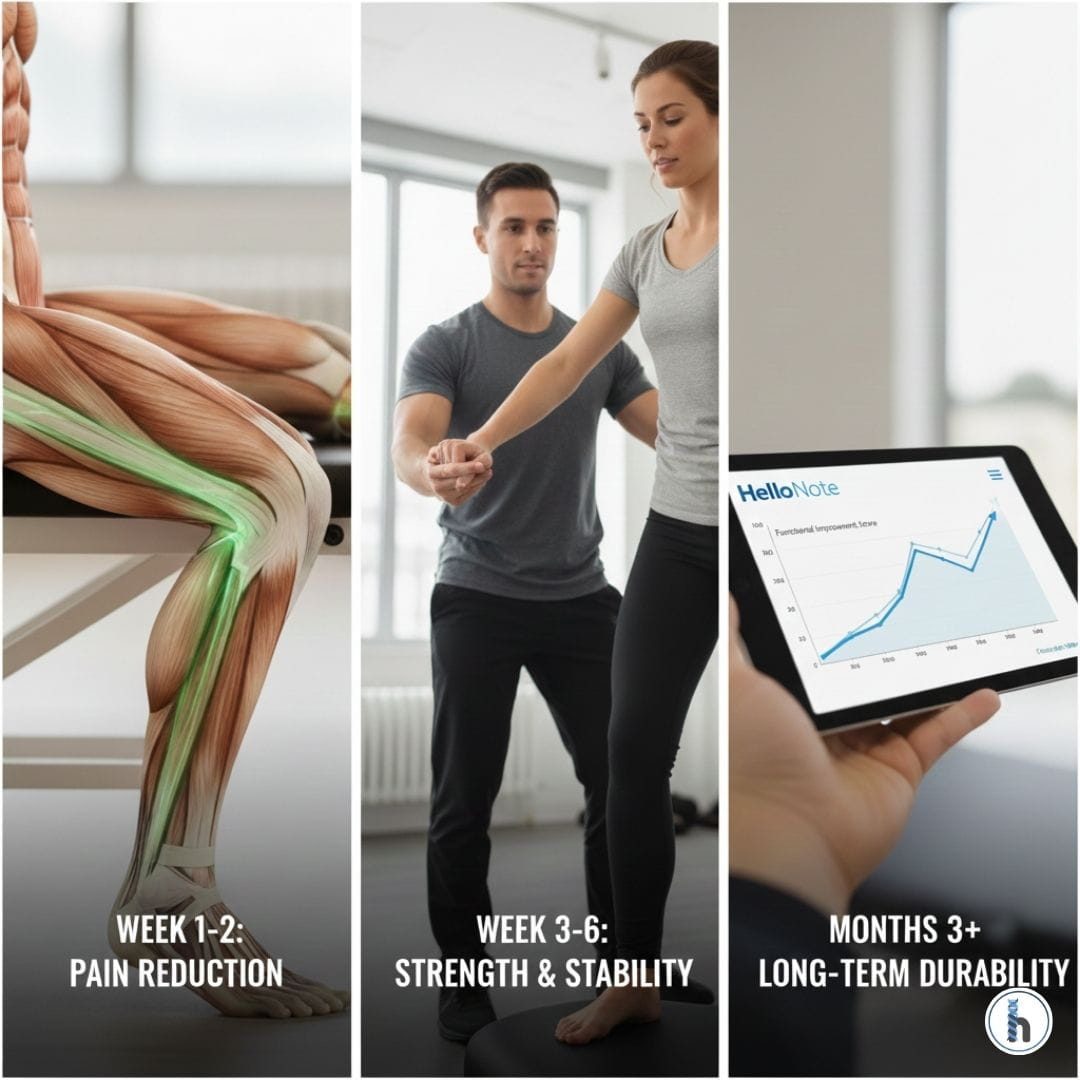
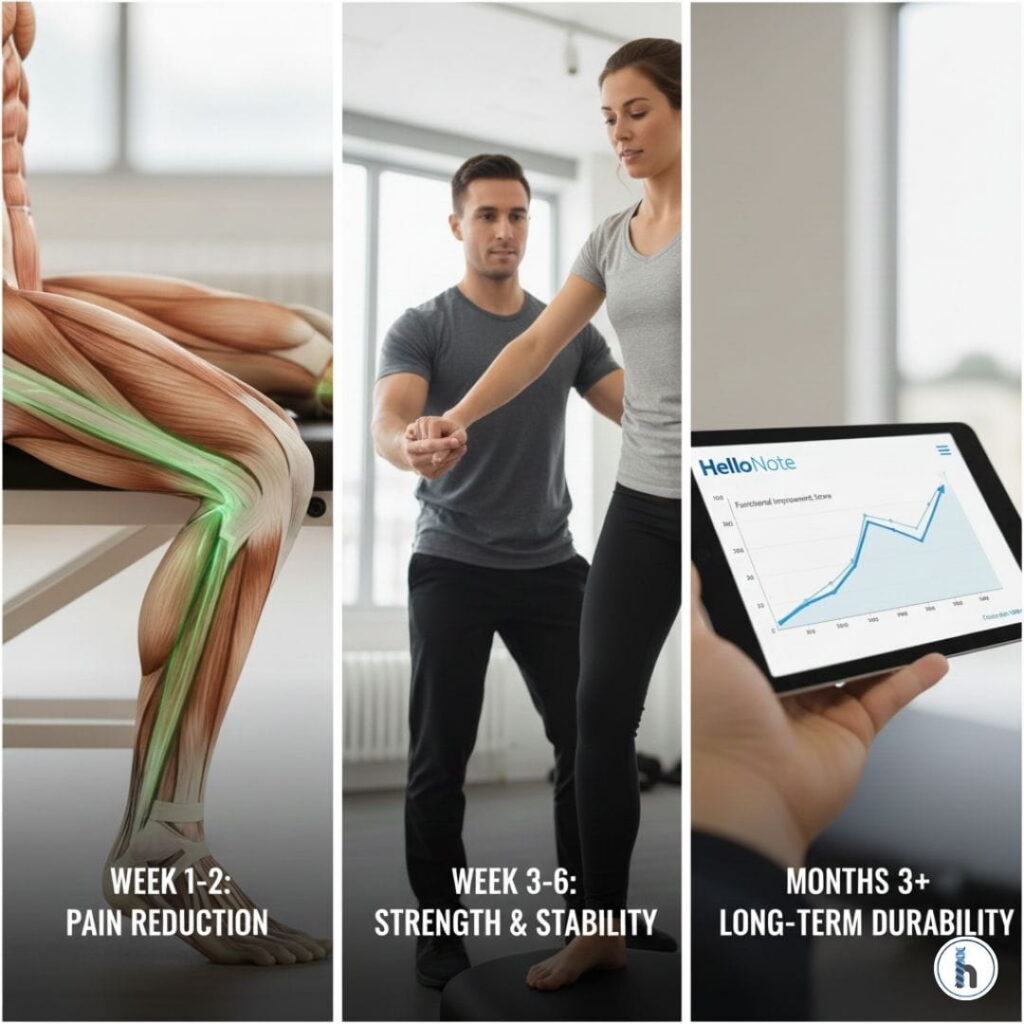
Most patients experience measurable pain reduction and mobility improvements within 2 to 4 weeks of consistent physical therapy. However, meaningful functional recovery—the kind that restores strength, stability, and durability—typically requires 6 to 12 weeks for most orthopedic injuries and 3 to 6 months for post-surgical rehabilitation.
The Biology of Recovery: Understanding Tissue “Speed Limits”
Recovery is governed by physiology, not motivation. The key variable is vascularity (blood supply). Tissues with rich blood flow heal faster; tissues with limited blood supply require longer remodeling phases.
Muscle (2–4 Weeks)
Highly vascular: Rapid cellular turnover.
Responds quickly: Progressive loading helps muscle strains feel better within weeks—but strengthening must continue beyond pain resolution.
Tendons & Ligaments (6–12 Weeks)
-
-
Limited blood supply: Heal through mechanotransduction (graded loading stimulates collagen repair).
-
The Risk: This is where most patients quit too early. Pain often decreases by week 4, but structural remodeling continues for months.
-
Cartilage (12+ Weeks)
No direct blood supply: Relies on joint compression and decompression for nutrient exchange. Therapy focuses on load management and symptom control, not true structural regeneration.
The Remodeling Reality in 2026
Research continues to confirm: Pain reduction ≠ full healing. Peak tensile strength of injured tissue may take up to 1–2 years. The most common cause of re-injury in 2026 remains: Stopping therapy once pain is gone.
2026 Recovery Timeline Estimates by Condition
| Injury Type | Initial Relief | Functional Progress | Full Recovery |
| Muscle Strain | 3–7 Days | 2–3 Weeks | 4–6 Weeks |
| Ligament Sprain | 1–2 Weeks | 3–4 Weeks | 6–12 Weeks |
| Post-Surgical (TKA/THA) | 1–3 Weeks | 6–12 Weeks | 3–6 Months |
| Chronic Low Back Pain | 2–4 Weeks | 8–12 Weeks | Ongoing Mgmt |
The Therapist’s Insight: The “Two-Week Rule”
Week 2 is pivotal. Patients either feel better and think they are cured, or they don’t feel 100% and doubt the process. I use the first two weeks to calm inflammation and restore mobility, but I clearly explain: “Weeks 1–2 calm things down. Weeks 3–6 build things up.”
Objective Progress Changes Behavior
Subjective pain fluctuates, but objective metrics do not.
Using HelloNote’s outcome tracking, therapists can document range-of-motion improvements, track strength gains, and record functional outcome score changes (e.g., Oswestry, DASH, LEFS). When a patient sees improved gait symmetry or lower disability scores, they remain engaged. Data reduces dropout.
Red Flags: When Recovery Plateaus
If a patient plateaus for more than 3 weeks, it is a clinical signal. In 2026, therapists look beyond the joint:
Evaluate sleep quality and protein intake (~1.2g/kg).
Assess systemic inflammation and psychosocial stressors.
Check exercise dosing errors.
When Should Diagnosis Be Reassessed?
If there is zero improvement in 3 weeks, or increasing neurological symptoms, it may require advanced imaging, physician referral, or multidisciplinary care.
Insurance & Documentation in 2026
Medicare and other payers require documented proof of “significant functional progress,” typically reassessed every 10 visits. HelloNote supports this through:
Automated Outcome Measures: Calculates scores tied to medical necessity.
Trend Analytics: Visualizes trajectory to justify continued care.
HEP Adherence Logs: Links patient compliance to outcomes.
Frequently Asked Questions
Recovery depends on age, biological baseline, fitness, and comorbidities. Comparison is rarely clinically relevant.
Not necessarily. Tissues require 24–48 hours between heavy loading sessions. Overtraining can restart the inflammatory phase and delay progress.
Lack of change is data—not failure. It requires a diagnosis review, loading strategy modification, or referral consideration.
No. Generic exercises online are not tailored to your specific biomechanical needs or tissue healing phase. Performing the wrong exercise at the wrong time can lead to compensation patterns or re-injury. A professional physical therapist ensures your loading strategy matches your body’s current biological recovery phase, which is critical for long-term durability.
Insurance coverage is typically tied to “medical necessity” and functional progress rather than a specific end-date or total symptom resolution. Payers expect documented improvements in function. If progress stalls, coverage may be reviewed. HelloNote helps therapists maintain the rigorous documentation required to justify continued care based on objective functional data.